

Optimal timing of antenatal corticosteroid administration and preterm neonatal and early childhood outcomes
- PMID: 32905377
- PMCID: PMC7469940
- DOI: 10.1016/j.ajogmf.2019.100077
Optimal timing of antenatal corticosteroid administration and preterm neonatal and early childhood outcomes
Abstract
Background: Antenatal corticosteroids reduce morbidity and mortality among preterm neonates. However, the optimal timing of steroid administration with regards to severe neonatal and early childhood morbidity is uncertain.
Objective: To evaluate the association between the timing of antenatal corticosteroid adminstration and preterm outcomes. We hypothesized that neonates exposed to antenatal corticosteroids 2 to <7 days before delivery would have the lowest risks of neonatal and childhood morbidity.
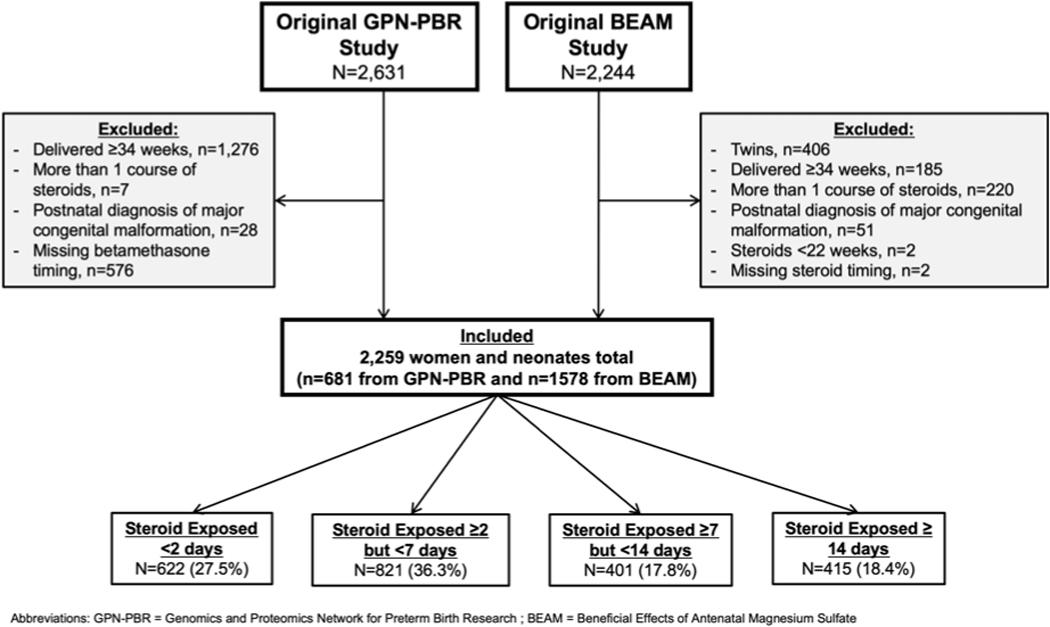
Study design: Secondary analysis of two prospective multicenter studies enriched for spontaneous preterm birth, Genomics and Proteomics Network for Preterm Birth Research (11/2007-1/2011) and Beneficial Effect of Antenatal Magnesium (12/1997-5/2004). We included women with singleton gestations who received antenatal corticosteroids and delivered at 23 0/7-33 6/7 weeks' gestation. Women who received ≥1 course of corticosteroids were excluded. Neonatal outcomes were compared by the timing of the first dose of antenatal corticosteroids in relation to delivery: <2 days, 2 to <7 days, 7 to <14 days, and ≥14 days. The primary outcome was respiratory distress syndrome. Secondary outcomes included composite neonatal morbidity (death, intraventricular hemorrhage grade III or IV, periventricular leukomalacia, bronchopulmonary dysplasia, or necrotizing enterocolitis), and early childhood morbidity (death or moderate to severe cerebral palsy at age 2). Multivariable logistic regression estimated the association between timing of antenatal corticosteroid administration and study outcomes.
Results: A total of 2,259 subjects met inclusion criteria: 622 (27.5%) received antenatal corticosteroids <2 days before delivery, 821 (36.3%) 2 to <7 days, 401 (17.8%) 7 to <14 days, and 415 (18.4%) ≥14 days. The majority (78.1%) delivered following idiopathic spontaneous preterm labor or preterm premature rupture of membranes at a mean gestational age of 29.5 +/-2.8 weeks. Neonates exposed to antenatal corticosteroids 2 to <7 days before delivery were the least likely to develop respiratory distress syndrome (51.3%), compared to those receiving antenatal corticosteroids <2 days, 7 to <14 days, and ≥14 days before delivery (62.7%, 55.9%, and 57.6%, respectively, p<0.001). Compared to receipt 2 to <7 days before delivery, there was an increased odds of respiratory distress syndrome with receipt of antenatal corticosteroids <2 days (aOR 2.07, 95%CI 1.61-2.66), 7 to <14 days (aOR 1.40, 95% CI 1.07-1.83), and ≥14 days (aOR 2.34, 95%CI 1.78-3.07). Neonates exposed to antenatal corticosteroids ≥14 days before delivery were at increased odds for severe neonatal morbidity (aOR 1.57, 95%CI 1.12-2.19) and early childhood morbidity (aOR 1.74, 95%CI 1.02-2.95), compared to those exposed 2 to <7 days before delivery. There was no significant association between antenatal corticosteroid receipt <2 days or 7 to <14 days and severe neonatal morbidity or severe childhood morbidity.
Conclusions: Preterm neonates exposed to antenatal corticosteroids 2 to <7 days before delivery had the lowest odds of respiratory distress syndrome, compared to shorter and longer time intervals between steroid administration and delivery. Antenatal corticosteroid administration ≥14 days before delivery is associated with an increased odds of severe neonatal and childhood morbidity, compared to 2 to <7 days before delivery. These results emphasize the importance of optimally timed antenatal corticosteroids to improve both short- and long-term outcomes.
Keywords: antenatal corticosteroids; childhood morbidity; neonatal morbidity; preterm birth; respiratory distress syndrome.
Similar articles
-
Time interval from late preterm antenatal corticosteroid administration to delivery and the impact on neonatal outcomes.Am J Obstet Gynecol MFM. 2021 Sep;3(5):100426. doi: 10.1016/j.ajogmf.2021.100426. Epub 2021 Jun 18. Am J Obstet Gynecol MFM. 2021. PMID: 34153514
-
One vs 2 courses of antenatal corticosteroids in pregnancies at risk of preterm birth: a secondary analysis of the MACS trial.Am J Obstet Gynecol MFM. 2023 Jul;5(7):101002. doi: 10.1016/j.ajogmf.2023.101002. Epub 2023 May 4. Am J Obstet Gynecol MFM. 2023. PMID: 37149145 Clinical Trial.
-
Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth.Cochrane Database Syst Rev. 2020 Dec 25;12(12):CD004454. doi: 10.1002/14651858.CD004454.pub4. Cochrane Database Syst Rev. 2020. PMID: 33368142 Free PMC article.
-
Implementation of an antenatal late-preterm corticosteroid protocol at a high-volume tertiary care center.Am J Obstet Gynecol MFM. 2020 Feb;2(1):100076. doi: 10.1016/j.ajogmf.2019.100076. Epub 2019 Dec 17. Am J Obstet Gynecol MFM. 2020. PMID: 32944712 Free PMC article.
-
Antenatal corticosteroids in preterm small-for-gestational age infants: a systematic review and meta-analysis.Am J Obstet Gynecol MFM. 2020 Nov;2(4):100215. doi: 10.1016/j.ajogmf.2020.100215. Epub 2020 Aug 17. Am J Obstet Gynecol MFM. 2020. PMID: 33345924 Free PMC article.
Cited by
-
Exposure to medication for neurological disease in pregnancy - time to consider the long-term implications?EClinicalMedicine. 2023 Aug 24;63:102157. doi: 10.1016/j.eclinm.2023.102157. eCollection 2023 Sep. EClinicalMedicine. 2023. PMID: 37662523 Free PMC article. Review.
-
The Impact of Antenatal Corticosteroids on the Metabolome of Preterm Newborns: An Untargeted Approach.Int J Mol Sci. 2024 May 28;25(11):5860. doi: 10.3390/ijms25115860. Int J Mol Sci. 2024. PMID: 38892043 Free PMC article.
-
Effect of dexamethasone on newborn survival at different administration-to-birth intervals: A secondary analysis of the WHO ACTION (Antenatal CorticosTeroids for Improving Outcomes in Preterm Newborn)-I trial.EClinicalMedicine. 2022 Nov 14;53:101744. doi: 10.1016/j.eclinm.2022.101744. eCollection 2022 Nov. EClinicalMedicine. 2022. PMID: 36467459 Free PMC article.
-
Evidence for the Management of Bronchopulmonary Dysplasia in Very Preterm Infants.Children (Basel). 2021 Apr 13;8(4):298. doi: 10.3390/children8040298. Children (Basel). 2021. PMID: 33924638 Free PMC article. Review.
-
Impact of antenatal corticosteroid therapy on neonatal outcomes in twin pregnancies.J Transl Med. 2025 Jul 3;23(1):739. doi: 10.1186/s12967-025-06679-w. J Transl Med. 2025. PMID: 40611291 Free PMC article.
References
-
- Martin JA, Hamilton BE, Osterman MJK, Driscoll AK, Mathews TJ. Births: Final Data for 2015. Natl Vital Stat Rep. 2017;66(1):1 http://www.ncbi.nlm.nih.gov/pubmed/28135188. Accessed November 13, 2018. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
