

Clinical Outcomes of Decompression Alone Versus and Decompression and Fusion for First Episode Recurrent Disc Herniation
- PMID: 32905723
- PMCID: PMC7485072
- DOI: 10.1177/2192568219878132
Clinical Outcomes of Decompression Alone Versus and Decompression and Fusion for First Episode Recurrent Disc Herniation
Abstract
Study design: Longitudinal cohort.
Objective: It is unclear if patients with a recurrent disc herniation benefit from a concurrent fusion compared with a repeat decompression alone. We compared outcomes of decompression alone (D0) versus decompression and fusion (DF) for recurrent disc herniation.
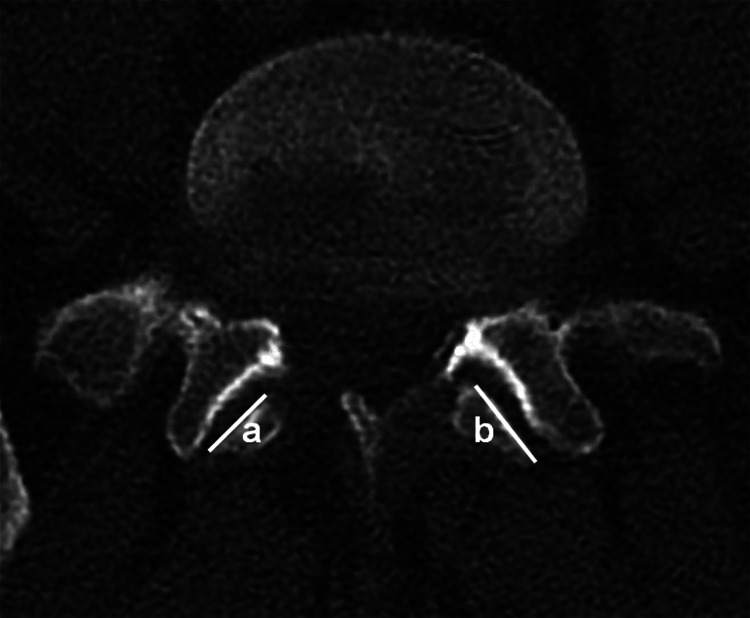
Methods: Patients enrolled in the Quality and Outcomes Database from 3 sites with a first episode of recurrent disc herniation were identified. Demographic, surgical, and radiographic data including the presence of listhesis and extent of facet resection on computed tomography or magnetic resonance imaging prior to the index surgery were collected. Patient-reported outcomes were collected preoperatively and at 3 and 12 months postoperatively.
Results: Of 94 cases identified, 55 had D0 and 39 had DF. Patients were similar in age, sex distribution, smoking status, body mass index, American Society of Anesthesiologists grade and surgical levels. Presence of listhesis (D0 = 7, DF = 5, P = .800) and extent of facet resection (D0 = 19%, DF = 16%, P = .309) prior to index surgery were similar between the 2 groups. Estimated blood loss (D0 = 26 cm3, DF = 329 cm3, P < .001), operating room time (D0 = 79 minutes, DF = 241 minutes, P < .001) and length of stay (D0 <1 day, DF = 4 days, P < .001) were significantly less in the D0 group. Preoperative and 1-year postoperative patient-reported outcomes were similar in both groups. Three patients in the D0 group and 2 patients in the DF group required revision. Regression analysis showed that presence of listhesis, extent of facet resection and fusion were not associated with the 12-month Oswestry Disability Index (ODI) score.
Conclusion: For a first episode recurrent disc herniation, surgeons can expect similar outcomes whether patients are treated with decompression alone or decompression and fusion.
Keywords: decompression and fusion; discectomy; patient-reported outcomes; recurrent disc herniation; decompression; revision surgery.
Conflict of interest statement
Figures
References
-
- Sonmez E, Coven I, Sahinturk F, Yilmaz C, Caner H. Unilateral percutaneous pedicle screw instrumentation with minimally invasive TLIF for the treatment of recurrent lumbar disk disease: 2 years follow-up. Turk Neurosurg. 2013;23:372–378. - PubMed
-
- Li Z, Tang J, Hou S, et al. Four-year follow-up results of transforaminal lumbar interbody fusion as revision surgery for recurrent lumbar disc herniation after conventional discectomy. J Clin Neurosci. 2015;22:331–337. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
