

NRG Oncology/RTOG Consensus Guidelines for Delineation of Clinical Target Volume for Intensity Modulated Pelvic Radiation Therapy in Postoperative Treatment of Endometrial and Cervical Cancer: An Update
- PMID: 32905846
- PMCID: PMC7856050
- DOI: 10.1016/j.ijrobp.2020.08.061
NRG Oncology/RTOG Consensus Guidelines for Delineation of Clinical Target Volume for Intensity Modulated Pelvic Radiation Therapy in Postoperative Treatment of Endometrial and Cervical Cancer: An Update
Abstract
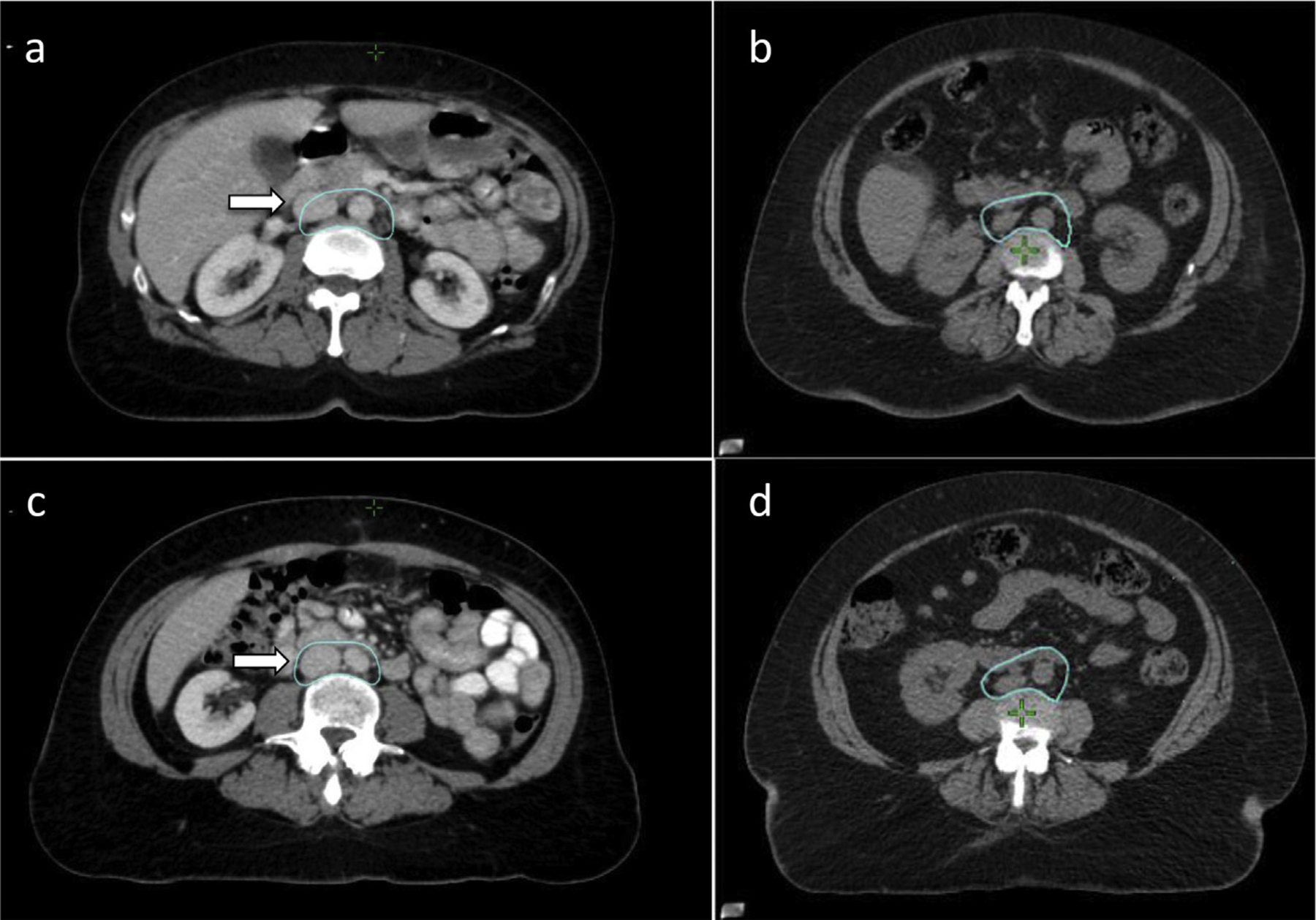
Purpose: Accurate target definition is critical for the appropriate application of radiation therapy. In 2008, the Radiation Therapy Oncology Group (RTOG) published an international collaborative atlas to define the clinical target volume (CTV) for intensity modulated pelvic radiation therapy in the postoperative treatment of endometrial and cervical cancer. The current project is an updated consensus of CTV definitions, with removal of all references to bony landmarks and inclusion of the para-aortic and inferior obturator nodal regions.
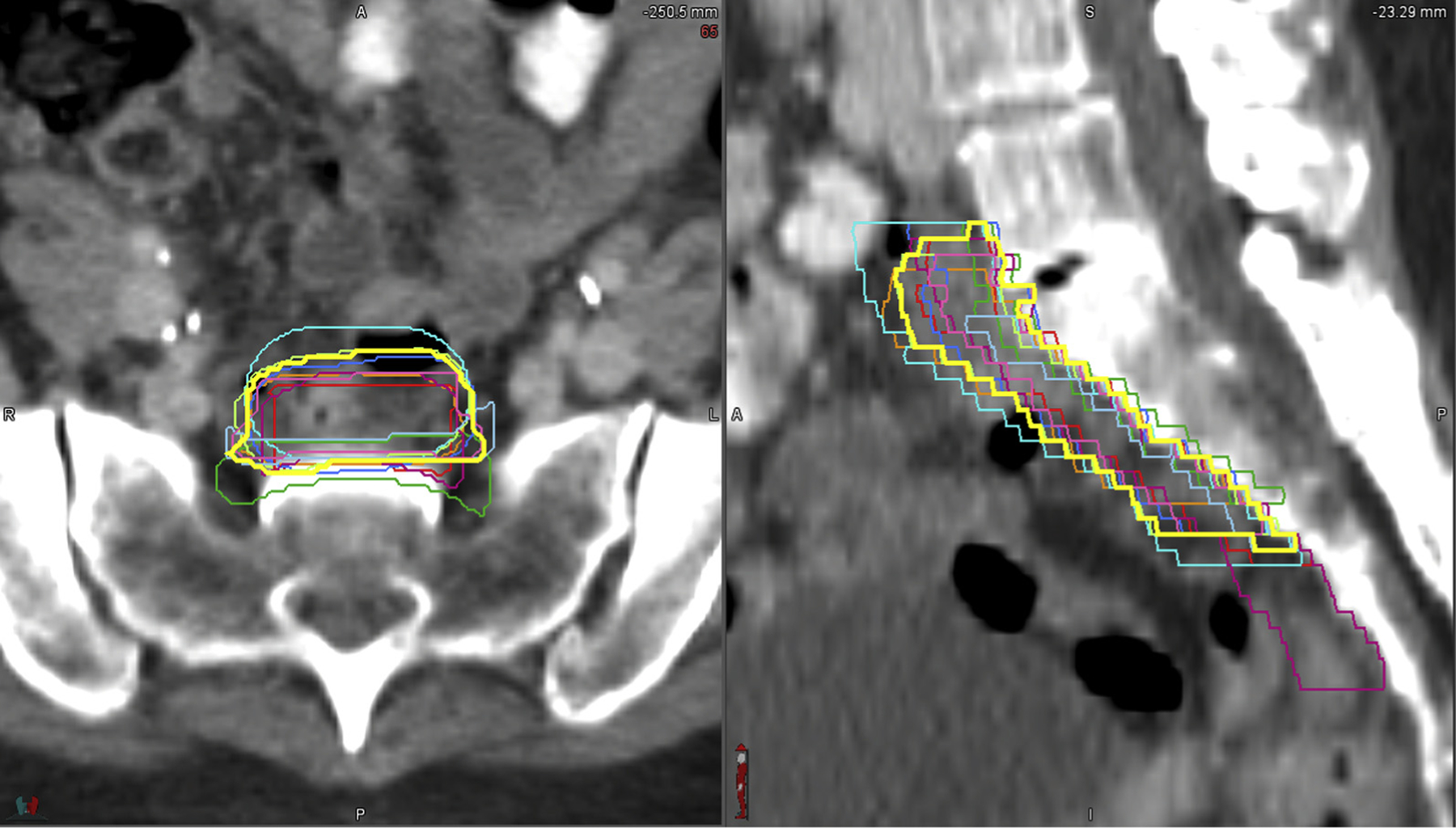
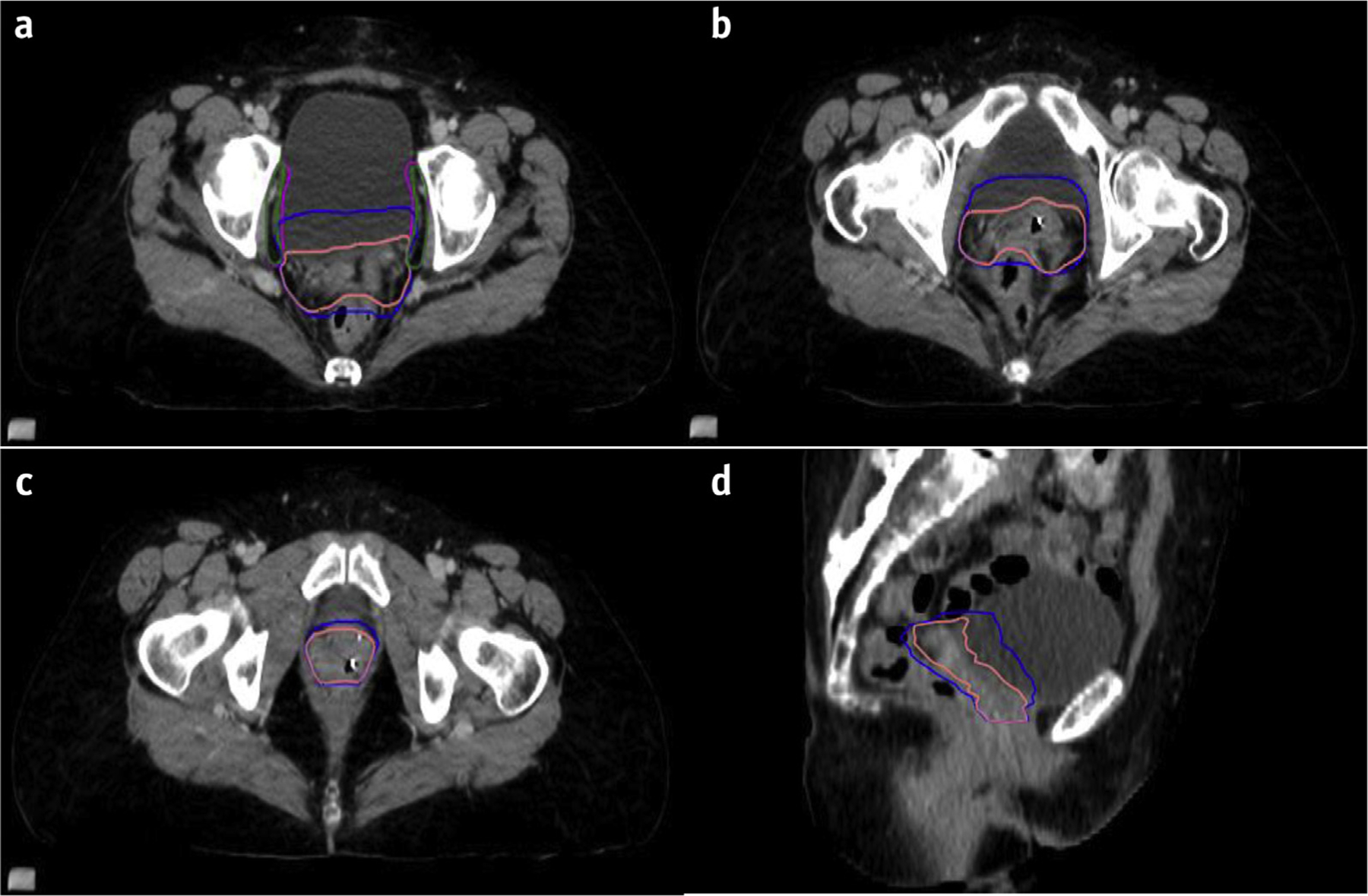
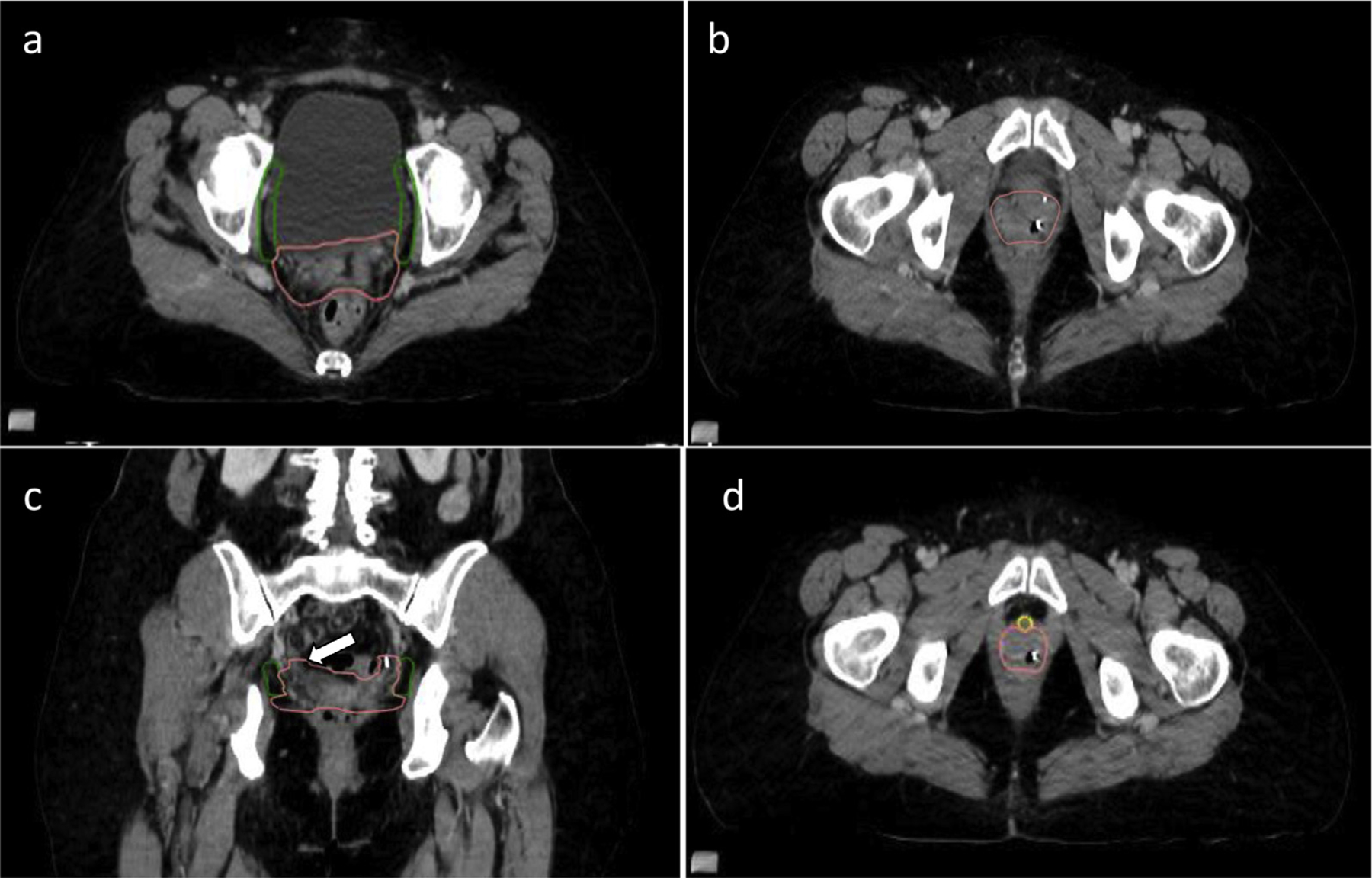
Methods and materials: An international consensus guideline working group discussed modifications of the current atlas and areas of controversy. A document was prepared to assist in contouring definitions. A sample case abdominopelvic computed tomographic image was made available, on which experts contoured targets. Targets were analyzed for consistency of delineation using an expectation-maximization algorithm for simultaneous truth and performance level estimation with kappa statistics as a measure of agreement between observers.
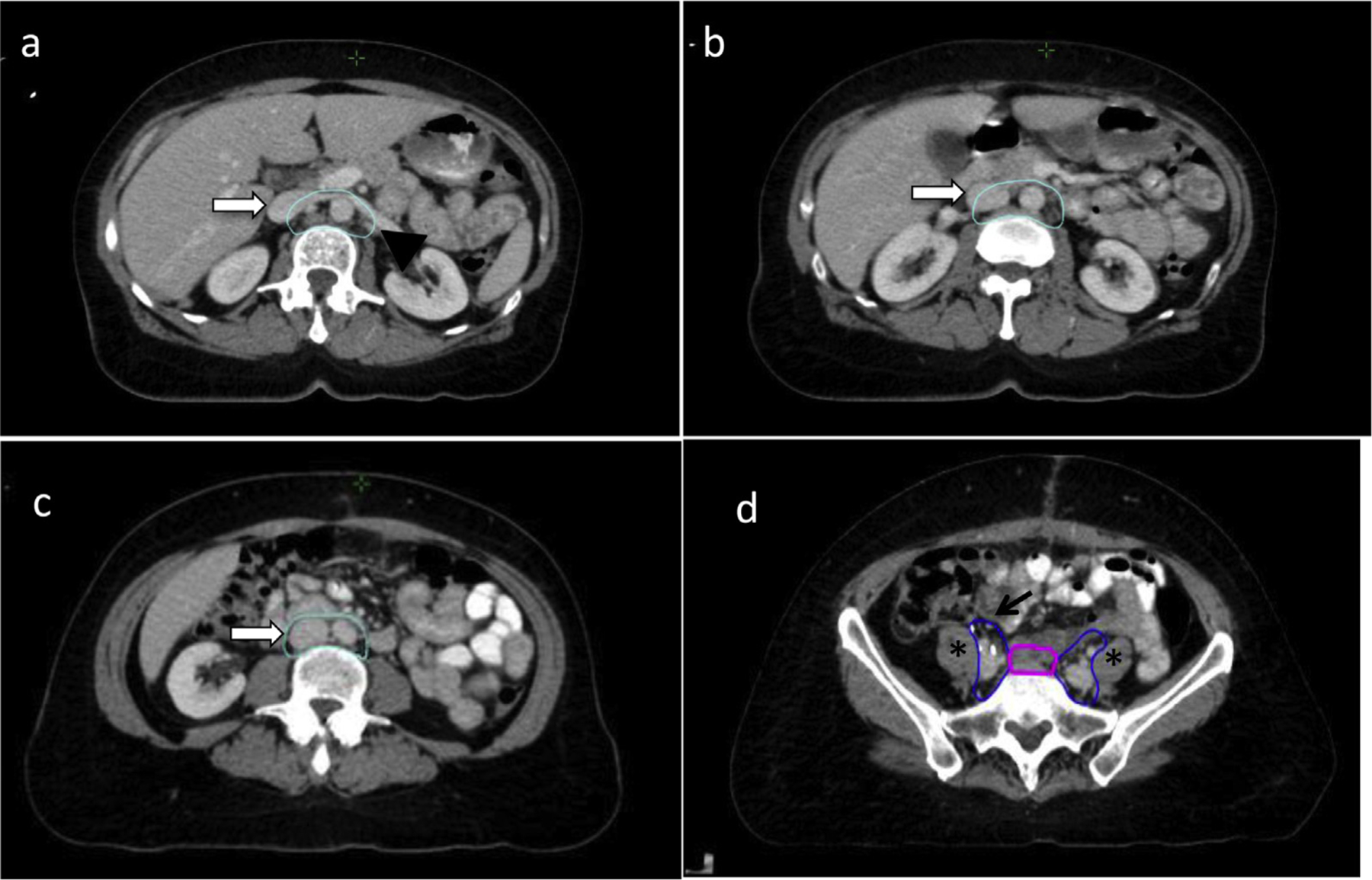
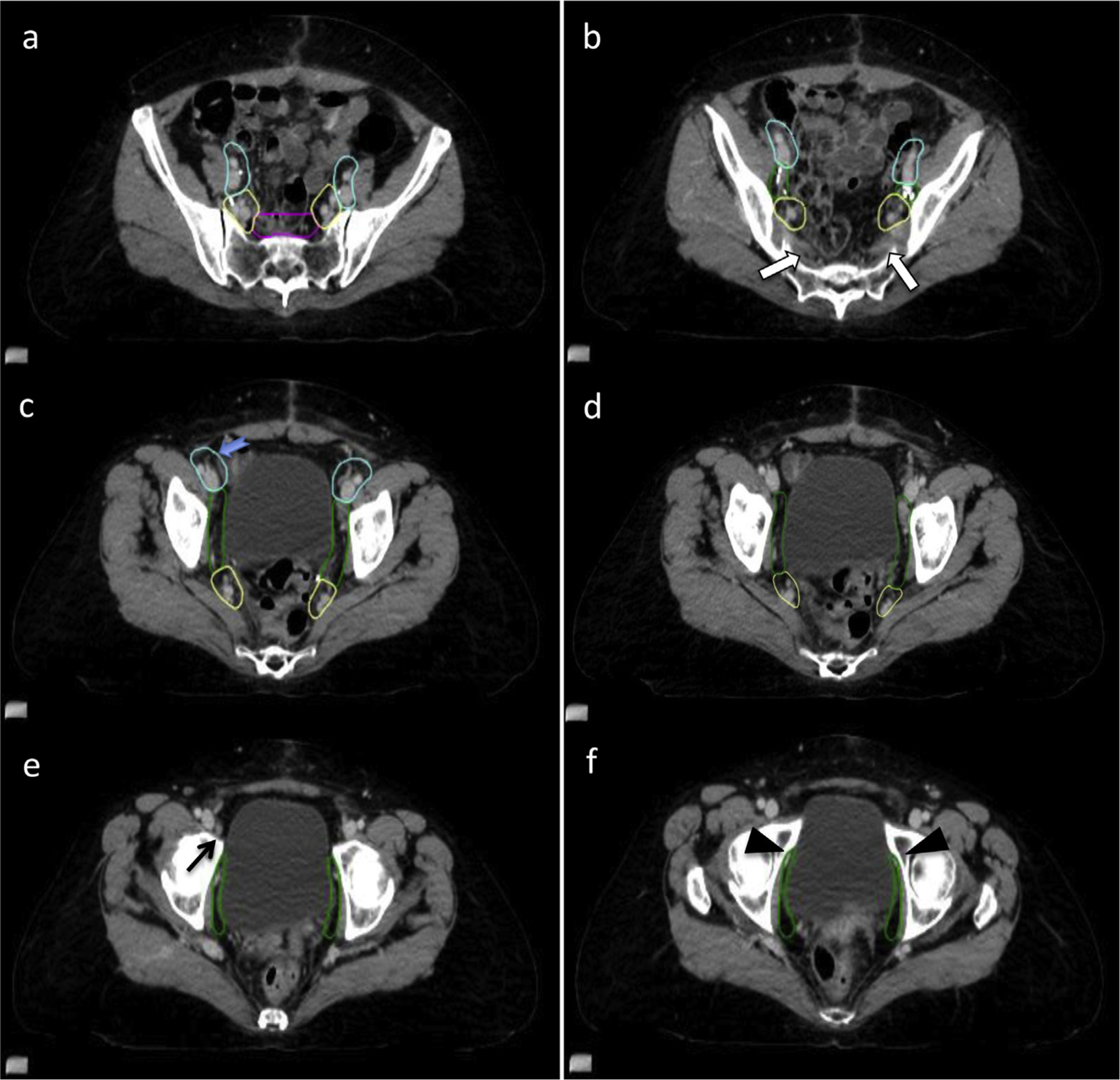
Results: Sixteen participants provided 13 sets of contours. Participants were asked to provide separate contours of the following areas: vaginal cuff, obturator, internal iliac, external iliac, presacral, common iliac, and para-aortic regions. There was substantial agreement for the common iliac region (sensitivity 0.71, specificity 0.981, kappa 0.64), moderate agreement in the external iliac, para-aortic, internal iliac and vaginal cuff regions (sensitivity 0.66, 0.74, 0.62, 0.59; specificity 0.989, 0.966, 0.986, 0.976; kappa 0.60, 0.58, 0.52, 0.47, respectively), and fair agreement in the presacral and obturator regions (sensitivity 0.55, 0.35; specificity 0.986, 0.988; kappa 0.36, 0.21, respectively). A 95% agreement contour was smoothed and a final contour atlas was produced according to consensus.
Conclusions: Agreement among the participants was most consistent in the common iliac region and least in the presacral and obturator nodal regions. The consensus volumes formed the basis of the updated NRG/RTOG Oncology postoperative atlas. Continued patterns of recurrence research are encouraged to refine these volumes.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
Comment in
-
In regard to Hall et al and Small et al.Int J Radiat Oncol Biol Phys. 2021 Mar 15;109(4):1125-1126. doi: 10.1016/j.ijrobp.2020.11.043. Int J Radiat Oncol Biol Phys. 2021. PMID: 33610294 No abstract available.
References
-
- Creasman WT, Morrow CP, Bundy BN, et al. Surgical pathologic spread patterns of endometrial cancer. A Gynecologic Oncology Group Study. Cancer 1987;60:2035–2041. - PubMed
-
- Creutzberg CL, van Putten WL, Koper PC, et al. Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: multicentre randomised trial. PORTEC Study Group. Post operative radiation therapy in endometrial carcinoma. Lancet 2000;355:1404–1411. - PubMed
-
- Keys HM, Roberts JA, Brunetto VL, et al. A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: a Gynecologic Oncology Group study. Gynecol Oncol 2004;92:744–751. - PubMed
-
- Greven K, Winter K, Underhill K, et al. Final analysis of RTOG 9708: adjuvant postoperative irradiation combined with cisplatin/paclitaxel chemotherapy following surgery for patients with high-risk endometrial cancer. Gynecol Oncol 2006;103:155–159. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
