

Management of Cardiac Toxicity Induced by Chemotherapy
- PMID: 32906611
- PMCID: PMC7565686
- DOI: 10.3390/jcm9092885
Management of Cardiac Toxicity Induced by Chemotherapy
Abstract
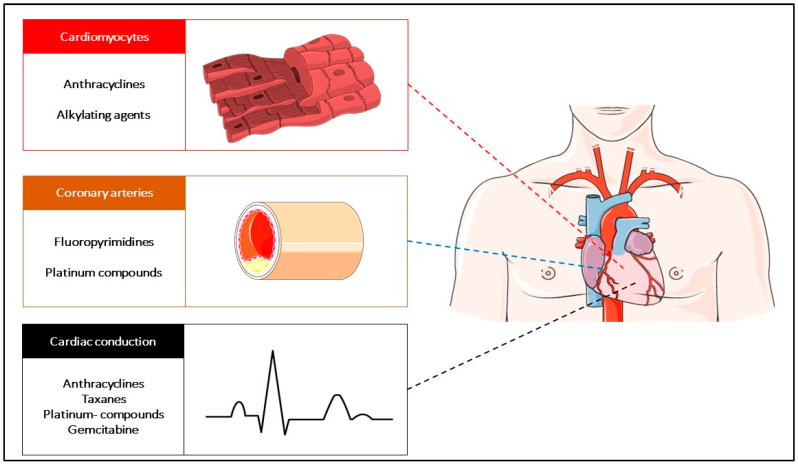
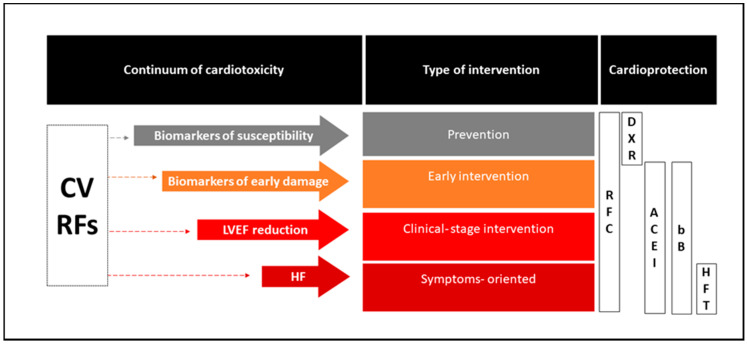
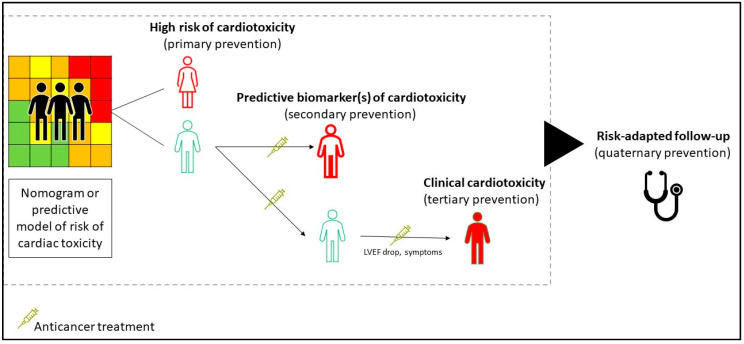
Cardiotoxicity encompasses a spectrum of adverse cardiological effects experienced by cancer patients during and after receiving antineoplastic treatments. The intersection of cancer care with the management of the multiple comorbid non-communicable diseases carried by patients or related to cancer treatments motivates the need for an integrated and multidisciplinary approach to therapeutic clinical decision-making. This present review aimed to provide a perspective and an update of the current pharmacotherapy approaches for the prevention and management of cardiotoxicity from antiblastic chemotherapy; as such, it addresses myocardial, vascular, and arrhythmic disorders associated to chemotherapy, by navigating the current knowledge and clinical indications in support of the medical interventions. Clinical scenarios of pharmacological interventions take place with patients receiving anthracycline and, by extrapolation, other agents with cardiotoxic potentials and non-chemotherapy agents, including various small molecules and immunotherapy agents. Analysis of these scenarios aims to provide practical evidence-based guidance for the management of drug-induced cardiac dysfunctions. The possible role of new biomarkers for the early recognition of cardiotoxicity is mentioned across the clinical studies, with reference to the pharmacological biomarker-driven interventions delivered. To best inform survivorship care, the management and context of cardio-oncology services are discussed within the broader network of providers and settings of care.
Keywords: cardio-oncology; cardiotoxicity; chemotherapy; pharmacotherapy; treatment-related adverse events.
Conflict of interest statement
G.C. has received honoraria from Pfizer, Novartis, Lilly, and Roche; fees for expert testimony and medical education from Pfizer; has participated in advisory boards for Pfizer, Roche, Lilly, Novartis, Seattle Genetics, and Celltrion. G.P., D.T., P.Z., and E.N. have no potential conflicts of interest to disclose regarding this paper. Although the declaration of interests has been provided to allow for the highest standard for transparency, the authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest for this specific work.
Figures
Similar articles
-
Rationale and design of the multidisciplinary team IntervenTion in cArdio-oNcology study (TITAN).BMC Cancer. 2016 Sep 15;16(1):733. doi: 10.1186/s12885-016-2761-8. BMC Cancer. 2016. PMID: 27629548 Free PMC article.
-
Chemotherapy-induced cardiotoxicity in children.Expert Opin Drug Metab Toxicol. 2017 Aug;13(8):817-832. doi: 10.1080/17425255.2017.1351547. Epub 2017 Jul 13. Expert Opin Drug Metab Toxicol. 2017. PMID: 28679288 Review.
-
Cardio-oncology - strategies for management of cancer-therapy related cardiovascular disease.Int J Cardiol. 2019 Apr 1;280:163-175. doi: 10.1016/j.ijcard.2019.01.038. Epub 2019 Jan 11. Int J Cardiol. 2019. PMID: 30661849 Review.
-
From cardio-oncology to cardio-onco-pharmacology: Towards a multidisciplinary approach in the understanding and management of cardiotoxicity.Therapie. 2022 Mar-Apr;77(2):197-206. doi: 10.1016/j.therap.2021.09.008. Epub 2021 Nov 25. Therapie. 2022. PMID: 34895759
-
Cardiotoxicity of anticancer treatments: Epidemiology, detection, and management.CA Cancer J Clin. 2016 Jul;66(4):309-25. doi: 10.3322/caac.21341. Epub 2016 Feb 26. CA Cancer J Clin. 2016. PMID: 26919165 Review.
Cited by
-
Personality Traits and Cardiotoxicity Arising From Cancer Treatments: An Hypothesized Relationship.Front Psychol. 2021 May 5;12:546636. doi: 10.3389/fpsyg.2021.546636. eCollection 2021. Front Psychol. 2021. PMID: 34025489 Free PMC article.
-
New Concepts in Cardio-Oncology.Cancer Treat Res. 2023;188:303-341. doi: 10.1007/978-3-031-33602-7_12. Cancer Treat Res. 2023. PMID: 38175351
-
Long-Term Effects of Pediatric Acute Lymphoblastic Leukemia Chemotherapy: Can Recent Findings Inform Old Strategies?Front Oncol. 2021 Oct 15;11:710163. doi: 10.3389/fonc.2021.710163. eCollection 2021. Front Oncol. 2021. PMID: 34722258 Free PMC article. Review.
-
Heart Failure With Reduced Ejection Fraction in a Patient With Erdheim-Chester Disease on Dabrafenib.JACC Case Rep. 2024 May 18;29(12):102374. doi: 10.1016/j.jaccas.2024.102374. eCollection 2024 Jun 19. JACC Case Rep. 2024. PMID: 38808127 Free PMC article.
-
Cancer Therapy-Related Pulmonary Hypertension: A Review of Mechanisms and Implications for Clinical Practice.Anatol J Cardiol. 2023 Jun;27(6):299-307. doi: 10.14744/AnatolJCardiol.2023.3013. Anatol J Cardiol. 2023. PMID: 37257013 Free PMC article. Review.
References
-
- GBD 2015 Risk Factors Collaborators Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease. Lancet. 2016;388:1659–1724. doi: 10.1016/S0140-6736(16)31679-8. - DOI - PMC - PubMed
