

Fetal Cardiac Interventions-Polish Experience from "Zero" to the Third World Largest Program
- PMID: 32906670
- PMCID: PMC7576494
- DOI: 10.3390/jcm9092888
Fetal Cardiac Interventions-Polish Experience from "Zero" to the Third World Largest Program
Abstract
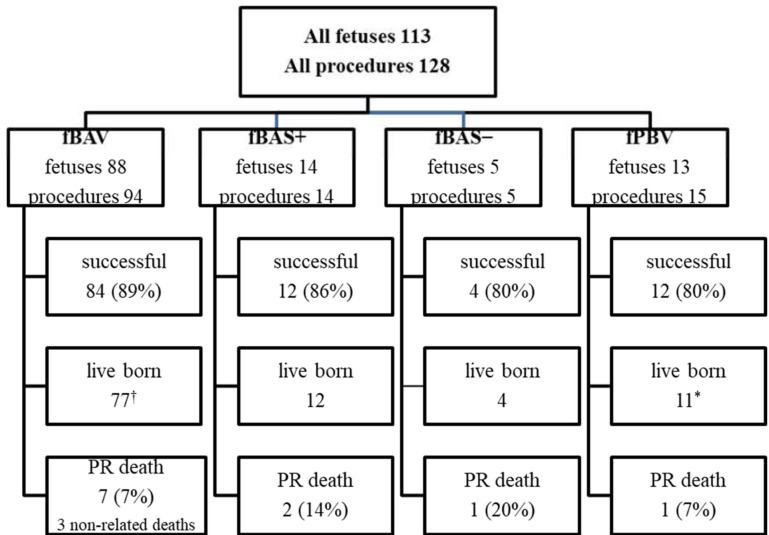
This article presents the technical aspects of the Polish fetal cardiac interventions (FCI) program, including preparation of the team and modifications in the technique of the procedure that aim to increase its safety for the mother and the fetus. Over 9 years, 128 FCI in 113 fetuses have been performed: 94 balloon aortic valvuloplasties (fBAV), 14 balloon atrioseptoplasties (fBAS) with stent (BAS+), 5 balloon atrioseptoplasties without stent placement (BAS-), and 15 fetal pulmonary valvuloplasties (fBPS). The technical success rate ranged from 80% (BAS-) to 89% (fBAV), while the procedure-related death rate (defined as death within 72 hours following the procedure) ranged from 7% (fBAV and fBPV) to 20% (BAS). There were 98 live births after all FCI (3 pregnancies continue). Median gestational age at delivery was 39 weeks in our center and 38 weeks in other centers.
Keywords: critical aortic stenosis; fetal cardiac interventions; fetal echocardiography; fetal valvuloplasty; hypoplastic left heart syndrome; pulmonary atresia and intact ventricular septum; technical aspects.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



Similar articles
-
Fetal Cardiac Interventions-Are They Safe for the Mothers?J Clin Med. 2021 Feb 19;10(4):851. doi: 10.3390/jcm10040851. J Clin Med. 2021. PMID: 33669554 Free PMC article.
-
[Prenatal interventional therapy in two cases with critical pulmonary stenosis or pulmonary atresia with intact ventricular septum].Zhonghua Er Ke Za Zhi. 2018 Jun 2;56(6):445-450. doi: 10.3760/cma.j.issn.0578-1310.2018.06.008. Zhonghua Er Ke Za Zhi. 2018. PMID: 29886608 Chinese.
-
Immediate effects and outcome of in-utero pulmonary valvuloplasty in fetuses with pulmonary atresia with intact ventricular septum or critical pulmonary stenosis.Ultrasound Obstet Gynecol. 2018 Aug;52(2):230-237. doi: 10.1002/uog.19047. Ultrasound Obstet Gynecol. 2018. PMID: 29569770 Free PMC article.
-
The boundaries of fetal cardiac intervention: Expand or tighten?Semin Fetal Neonatal Med. 2017 Dec;22(6):399-403. doi: 10.1016/j.siny.2017.08.006. Epub 2017 Sep 1. Semin Fetal Neonatal Med. 2017. PMID: 28867155 Review.
-
Catheter-Based Fetal Cardiac Interventions.J Cardiovasc Dev Dis. 2024 May 29;11(6):167. doi: 10.3390/jcdd11060167. J Cardiovasc Dev Dis. 2024. PMID: 38921667 Free PMC article. Review.
Cited by
-
Valvuloplasty in 103 fetuses with critical aortic stenosis: outcome and new predictors for postnatal circulation.Ultrasound Obstet Gynecol. 2022 May;59(5):633-641. doi: 10.1002/uog.24792. Epub 2022 Apr 11. Ultrasound Obstet Gynecol. 2022. PMID: 34605096 Free PMC article.
-
Hypoplastic Left Heart Syndrome: Is There a Role for Fetal Therapy?Front Pediatr. 2022 Jul 8;10:944813. doi: 10.3389/fped.2022.944813. eCollection 2022. Front Pediatr. 2022. PMID: 35874565 Free PMC article. Review.
-
Seasonality of Hypoplastic Left Heart Syndrome and Single Ventricle Heart in Poland in the Context of Air Pollution.J Clin Med. 2021 Jul 21;10(15):3207. doi: 10.3390/jcm10153207. J Clin Med. 2021. PMID: 34361990 Free PMC article.
-
Fetal Cardiac Interventions-Are They Safe for the Mothers?J Clin Med. 2021 Feb 19;10(4):851. doi: 10.3390/jcm10040851. J Clin Med. 2021. PMID: 33669554 Free PMC article.
-
Impact of fetal pulmonary valvuloplasty in in-utero critical pulmonary stenosis: A systematic review and meta-analysis.Int J Cardiol Congenit Heart Dis. 2023 Nov 18;15:100485. doi: 10.1016/j.ijcchd.2023.100485. eCollection 2024 Mar. Int J Cardiol Congenit Heart Dis. 2023. PMID: 39713496 Free PMC article.
References
-
- Moon-Grady A.J., Morris S.A., Belfort M., Chmait R., Dangel J., Devlieger R., Emery S., Frommelt M., Galindo A., Gelehrter S., et al. International Fetal Cardiac Intervention Registry: A Worldwide Collaborative Description and Preliminary Outcomes. J. Am. Coll. Cardiol. 2015;66:388–399. doi: 10.1016/j.jacc.2015.05.037. - DOI - PubMed
-
- Mäkikallio K., McElhinney D.B., Levine J.C., Marx G.R., Colan S.D., Marshall A.C., Lock J.E., Marcus E.N., Tworetzky W. Fetal Aortic Valve Stenosis and the Evolution of Hypoplastic Left Heart Syndrome: Patient Selection for Fetal Intervention. Circulation. 2006;113:1401–1405. doi: 10.1161/CIRCULATIONAHA.105.588194. - DOI - PubMed
-
- Kovacevic A., Öhman A., Tulzer G., Herberg U., Dangel J., Carvalho J.S., Fesslova V., Jicinska H., Sarkola T., Pedroza C., et al. Fetal Hemodynamic Response to Aortic Valvuloplasty and Postnatal Outcome: A European Multicenter Study. Ultrasound Obstet. Gynecol. 2018;52:221–229. doi: 10.1002/uog.18913. - DOI - PubMed
LinkOut - more resources
Full Text Sources
