

Aorto-Iliac Artery Calcification Prior to Kidney Transplantation
- PMID: 32906789
- PMCID: PMC7563260
- DOI: 10.3390/jcm9092893
Aorto-Iliac Artery Calcification Prior to Kidney Transplantation
Abstract
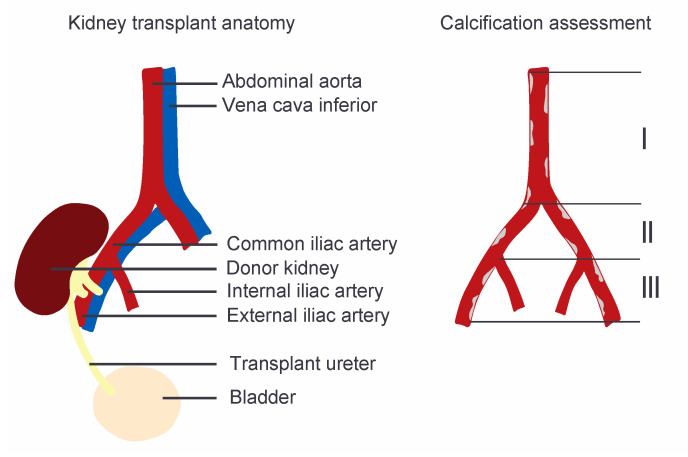
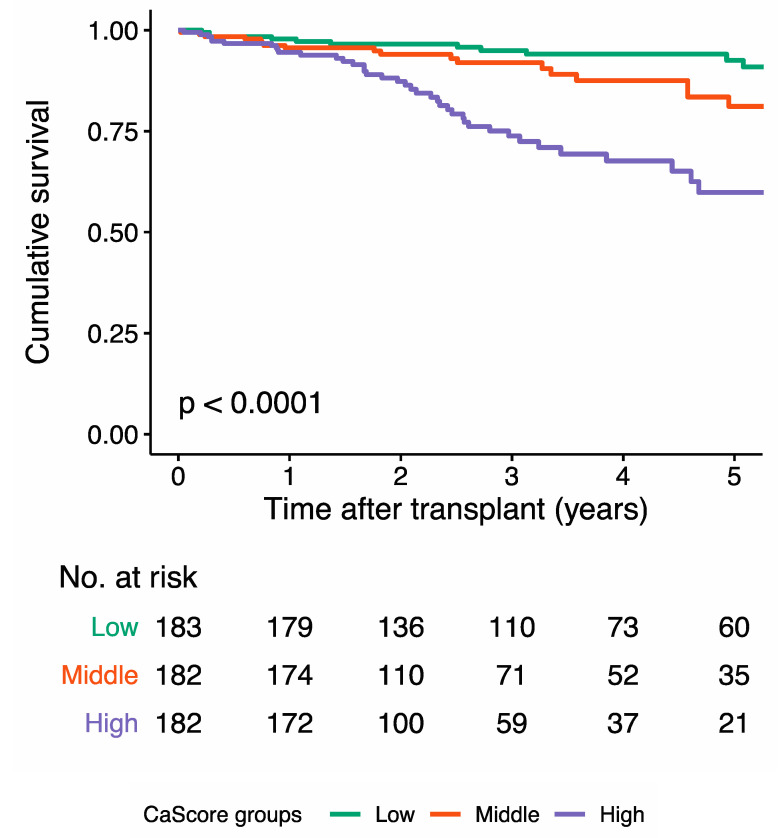
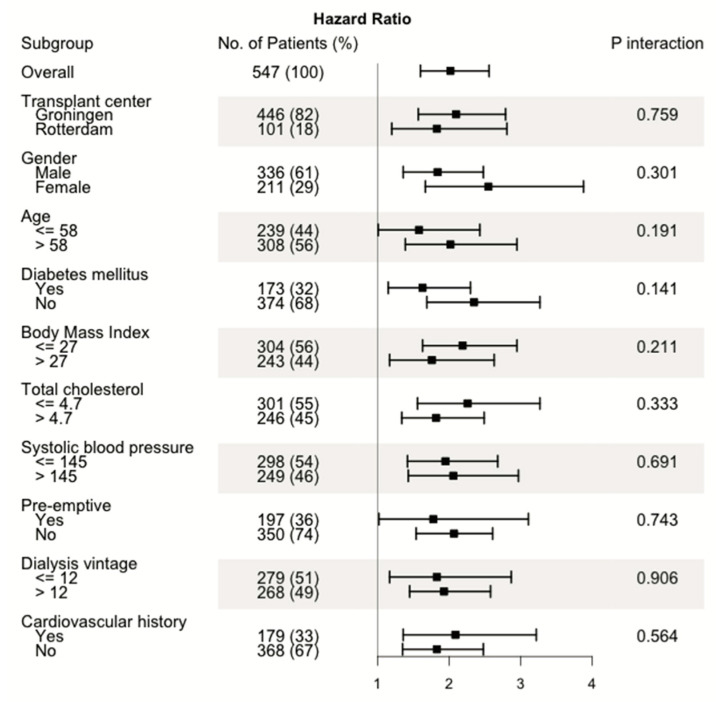
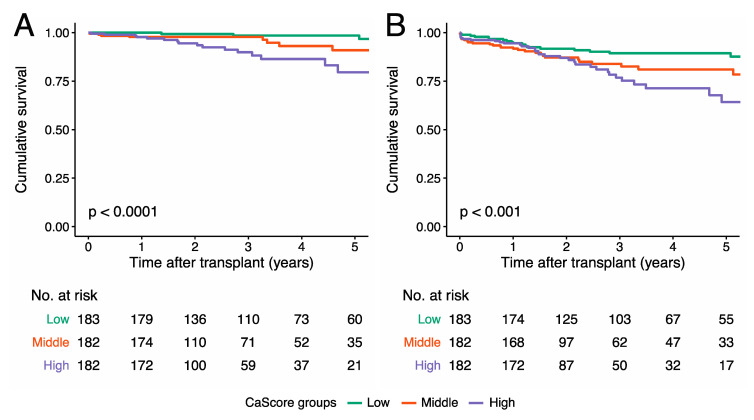
As vascular calcification is common in kidney transplant candidates, aorto-iliac vessel imaging is performed for surgical planning. The aim of the present study was to investigate whether a novel non-contrast enhanced computed tomography-based quantification technique for aorto-iliac calcification can be used for cardiovascular risk stratification prior to kidney transplantation. In this dual-center cohort study, we measured the aorto-iliac calcium score (CaScore) of 547 patients within three years prior to transplantation (2005-2018). During a median (interquartile range) follow-up of 3.1 (1.4, 5.2) years after transplantation, 80 (14.7%) patients died, of which 32 (40.0%) died due to cardiovascular causes, and 84 (15.5%) patients had a cardiovascular event. Kaplan-Meier survival curves showed significant differences between the CaScore tertiles for cumulative overall-survival (Log-rank test p < 0.0001), cardiovascular survival (p < 0.0001), and cardiovascular event-free survival (p < 0.001). In multivariable Cox regression, the aorto-iliac CaScore was associated with all-cause mortality (hazard ratio 1.53, 95%CI 1.14-2.06, p = 0.005), cardiovascular mortality (2.04, 1.20-3.45, p = 0.008), and cardiovascular events (1.35, 1.01-1.80, p = 0.042). These independent associations of the aorto-iliac CaScore with the outcome measures can improve the identification of patients at risk for (cardiovascular) death and those who could potentially benefit from stringent cardiovascular monitoring to improve their prognosis after transplantation.
Keywords: aorta; cardiovascular diseases; iliac artery; kidney transplantation; vascular calcification.
Conflict of interest statement
The authors declare no conflict of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Rangaswami J., Mathew R.O., Parasuraman R., Tantisattamo E., Lubetzky M., Rao S., Yaqub M.S., Birdwell K.A., Bennett W., Dalal P., et al. Cardiovascular disease in the kidney transplant recipient: Epidemiology, diagnosis and management strategies. Nephrol. Dial. Transplant. 2019;34:760–773. doi: 10.1093/ndt/gfz053. - DOI - PubMed
-
- Harhay M.N., Rao M.K., Woodside K.J., Johansen K.L., Lentine K.L., Tullius S.G., Parsons R.F., Alhamad T., Berger J., Cheng X.S., et al. An overview of frailty in kidney transplantation: Measurement, management and future considerations. Nephrol. Dial. Transplant. 2020;35:1099–1112. doi: 10.1093/ndt/gfaa016. - DOI - PMC - PubMed
-
- National Institute of Health. National Institute of Diabetes and Digestive and Kidney Diseases . United States Renal Data System 2017 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institute of Health; Bethesda, MD, USA: 2017.
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
