

Relationship between comprehensive geriatric assessment and amyloid PET in older persons with MCI
- PMID: 32907545
- PMCID: PMC7487621
- DOI: 10.1186/s12877-020-01746-x
Relationship between comprehensive geriatric assessment and amyloid PET in older persons with MCI
Abstract
Background: The association between amyloid deposition and cognitive, behavioral and physical performance in mild cognitive impairment (MCI) due to Alzheimer's disease (AD) has been poorly investigated, especially in older persons.
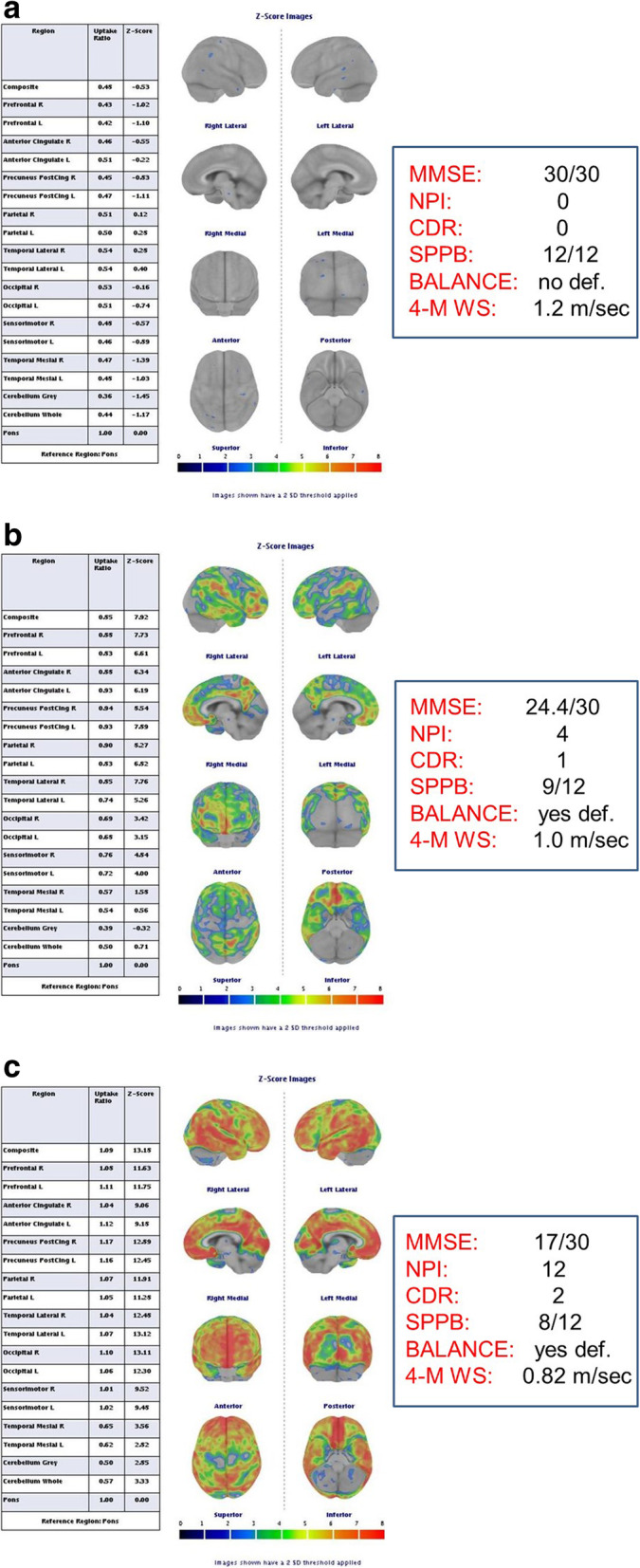
Methods: We studied the in vivo correlation between the amyloid deposition at Positron Emission Tomography (amyloid-PET) and the presence of memory loss, reduced executive function, neuropsychiatric symptoms and physical performance in older persons with MCI. Amyloid-PET was performed with 18F-flutemetamol and quantitatively analyzed.
Results: We evaluated 48 subjects, 21 men and 27 women. We performed in each patient a comprehensive geriatric assessment (CGA) including Mini Mental State Examination (MMSE), Clock Drawing Test (CDT), Activity Daily Living (ADL), Instrumental Activity of Daily Living (IADL), Neuropsychiatric inventory (NPI) questionnaire, 15 Geriatric Depression Scale (GDS), Short Physical Performance Battery (SPPB) and Hand Grip strength. Then, each patient underwent amyloid-PET. Mean age of the enrolled subjects was 74.6 ± 7.8 years. All of these subjects showed preserved cognitive function at MMSE > 24, while 29 of 48 subjects (61.0%) had altered CDT. Mean NPI score was 6.9 ± 5.9. The mean value of SPPB score was 9.0 ± 2.6, while the average muscle strength of the upper extremities measured by hand grip was 25.6 ± 7.7 Kg. CT/MRI images showed cortical atrophic changes in 26 of the 48 examined subjects (54.0%), while cerebrovascular modifications were present in 31 subjects (64.5%). Pathological burden of amyloid deposits was detected in 25 of 48 (52.0%) patients with a mean value of global z-score of 2.8 (subjects defined as MCI due to AD). After stratifying subjects in subclasses of clinical alterations, more probability of pathological amyloid deposition was found in subjects with impaired CDT and higher NPI score (O.R. = 3.45 [1.01-11.2], p = 0.04), with both impaired CDT and low physical performance (O.R. = 5.80 [1.04-32.2], p = 0.04), with altered CDT and high NPI score (O.R. = 7.98 [1.38-46.0], p = 0.02), and finally in those subjects with altered CDT, high NPI and low physical performance (O.R. = 5.80 [1.05-32.2], p = 0.04).
Conclusion: Our findings support the recent hypothesis that amyloid deposition could be associated with multiple cerebral dysfunction, mainly affecting executive, behavioral and motor abilities.
Keywords: Alzheimer’s disease; Amyloid deposition; MCI; Older persons; Physical performance; Positron emission tomography; motoric-cognitive risk syndrome.
Conflict of interest statement
None to declare.
Figures
References
-
- Alzheimer’s Association 2015 Alzheimer’s disease facts and figures. Alzheimers Dement. 2015;11(3):332–384. - PubMed
-
- GBD Disease and injury incidence and prevalence collaborators (2016) global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2015;388(10053):1545–1602. - PMC - PubMed
-
- Åkerborg Ö, Lang A, Wimo A, ei al (2016) Cost of dementia and its correlation with dependence. J Aging Health 28(8):1448–1464. - PubMed
-
- Scheltens P, Blennow K, Breteler MM, et al. Alzheimer’s disease. Lancet. 2016;388(10043):505–517. - PubMed
-
- Winblad B, Amouyel P, Andrieu S, et al. Defeating Alzheimer's disease and other dementias: a priority for European science and society. Lancet Neurol. 2016;15(5):455–532. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
