

Elevated D-dimers and lack of anticoagulation predict PE in severe COVID-19 patients
- PMID: 32907890
- PMCID: PMC7487272
- DOI: 10.1183/13993003.01811-2020
Elevated D-dimers and lack of anticoagulation predict PE in severe COVID-19 patients
Abstract
Background: Coronavirus disease 2019 (COVID-19) may predispose to venous thromboembolism. We determined factors independently associated with computed tomography pulmonary angiography (CTPA)-confirmed pulmonary embolism (PE) in hospitalised severe COVID-19 patients.
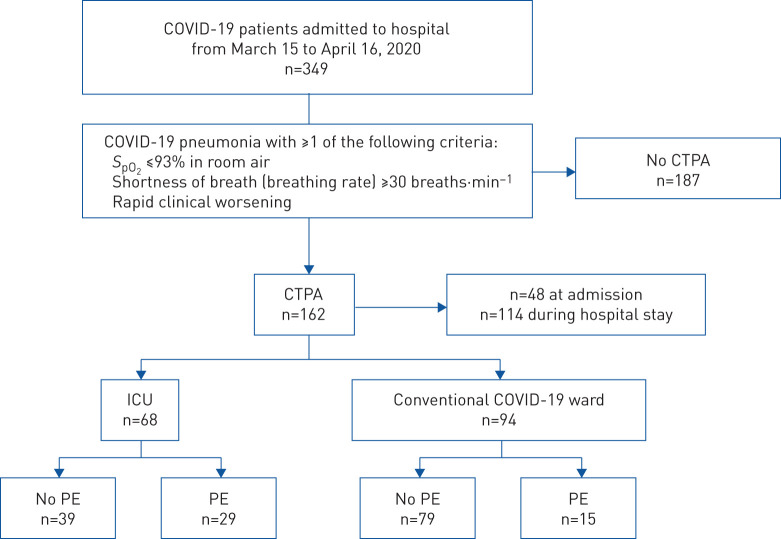
Methods: Among all (n=349) patients hospitalised for COVID-19 in a university hospital in a French region with a high rate of COVID-19, we analysed patients who underwent CTPA for clinical signs of severe disease (oxygen saturation measured by pulse oximetry ≤93% or breathing rate ≥30 breaths·min-1) or rapid clinical worsening. Multivariable analysis was performed using Firth penalised maximum likelihood estimates.
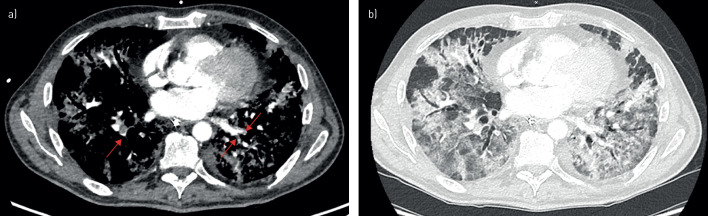
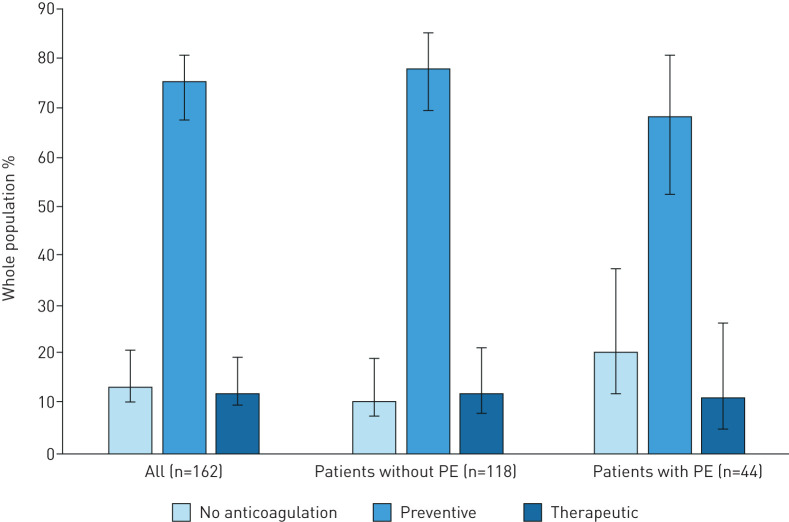
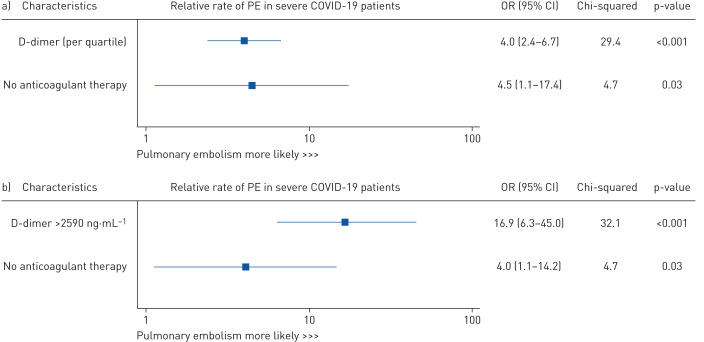
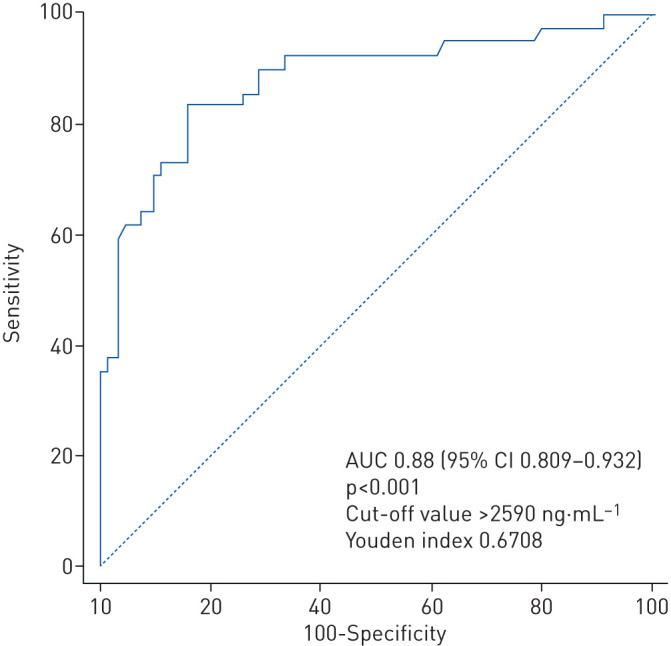
Results: 162 (46.4%) patients underwent CTPA (mean±sd age 65.6±13.0 years; 67.3% male (95% CI 59.5-75.5%). PE was diagnosed in 44 (27.2%) patients. Most PEs were segmental and the rate of PE-related right ventricular dysfunction was 15.9%. By multivariable analysis, the only two significant predictors of CTPA-confirmed PE were D-dimer level and the lack of any anticoagulant therapy (OR 4.0 (95% CI 2.4-6.7) per additional quartile and OR 4.5 (95% CI 1.1-7.4), respectively). Receiver operating characteristic curve analysis identified a D-dimer cut-off value of 2590 ng·mL-1 to best predict occurrence of PE (area under the curve 0.88, p<0.001, sensitivity 83.3%, specificity 83.8%). D-dimer level >2590 ng·mL-1 was associated with a 17-fold increase in the adjusted risk of PE.
Conclusion: Elevated D-dimers (>2590 ng·mL-1) and absence of anticoagulant therapy predict PE in hospitalised COVID-19 patients with clinical signs of severity. These data strengthen the evidence base in favour of systematic anticoagulation, and suggest wider use of D-dimer guided CTPA to screen for PE in acutely ill hospitalised patients with COVID-19.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: B. Mouhat has nothing to disclose. Conflict of interest: M. Besutti has nothing to disclose. Conflict of interest: K. Bouiller has nothing to disclose. Conflict of interest: F. Grillet has nothing to disclose. Conflict of interest: C. Monnin has nothing to disclose. Conflict of interest: F. Ecarnot has nothing to disclose. Conflict of interest: J. Behr has nothing to disclose. Conflict of interest: G. Capellier has nothing to disclose. Conflict of interest: T. Soumagne has nothing to disclose. Conflict of interest: S. Pili-Floury has nothing to disclose. Conflict of interest: G. Besch has nothing to disclose. Conflict of interest: G. Mourey has nothing to disclose. Conflict of interest: Q. Lepiller has nothing to disclose. Conflict of interest: C. Chirouze has nothing to disclose. Conflict of interest: F. Schiele has nothing to disclose. Conflict of interest: R. Chopard has nothing to disclose. Conflict of interest: N. Meneveau has nothing to disclose.
Figures
Comment in
-
How can we better predict pulmonary blood clots in patients hospitalised for COVID-19?Eur Respir J. 2020 Oct 22;56(4):2003092. doi: 10.1183/13993003.03092-2020. Print 2020 Oct. Eur Respir J. 2020. PMID: 32907888 Free PMC article.
-
Pulmonary embolism in COVID-19: D-dimer threshold selection should not be based on maximising Youden's index.Eur Respir J. 2021 Feb 4;57(2):2004279. doi: 10.1183/13993003.04279-2020. Print 2021 Feb. Eur Respir J. 2021. PMID: 33380510 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous