

COVID-19 and pneumothorax: a multicentre retrospective case series
- PMID: 32907891
- PMCID: PMC7487269
- DOI: 10.1183/13993003.02697-2020
COVID-19 and pneumothorax: a multicentre retrospective case series
Abstract
Introduction: Pneumothorax and pneumomediastinum have both been noted to complicate cases of coronavirus disease 2019 (COVID-19) requiring hospital admission. We report the largest case series yet described of patients with both these pathologies (including nonventilated patients).
Methods: Cases were collected retrospectively from UK hospitals with inclusion criteria limited to a diagnosis of COVID-19 and the presence of either pneumothorax or pneumomediastinum. Patients included in the study presented between March and June 2020. Details obtained from the medical record included demographics, radiology, laboratory investigations, clinical management and survival.
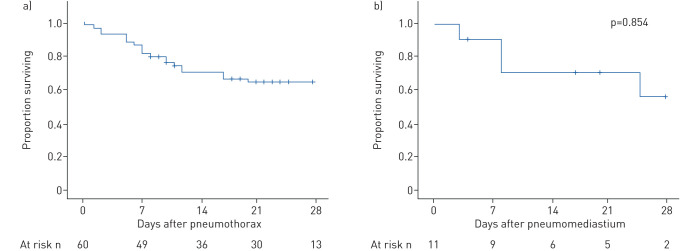
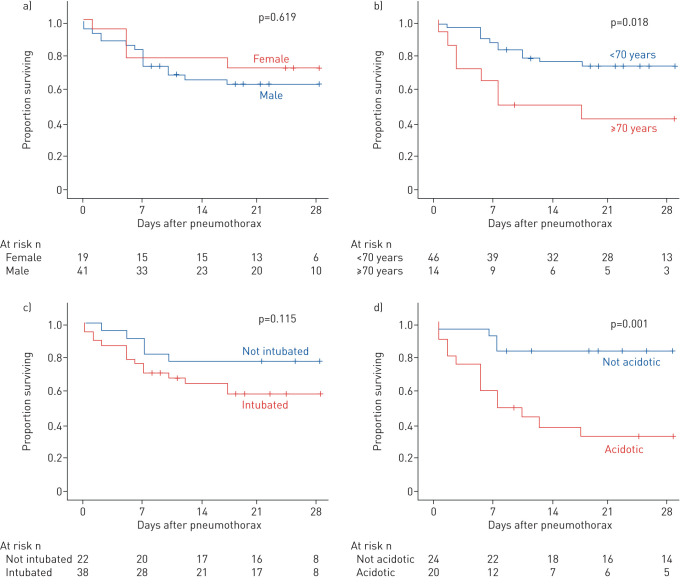
Results: 71 patients from 16 centres were included in the study, of whom 60 had pneumothoraces (six with pneumomediastinum in addition) and 11 had pneumomediastinum alone. Two of these patients had two distinct episodes of pneumothorax, occurring bilaterally in sequential fashion, bringing the total number of pneumothoraces included to 62. Clinical scenarios included patients who had presented to hospital with pneumothorax, patients who had developed pneumothorax or pneumomediastinum during their inpatient admission with COVID-19 and patients who developed their complication while intubated and ventilated, either with or without concurrent extracorporeal membrane oxygenation. Survival at 28 days was not significantly different following pneumothorax (63.1±6.5%) or isolated pneumomediastinum (53.0±18.7%; p=0.854). The incidence of pneumothorax was higher in males. 28-day survival was not different between the sexes (males 62.5±7.7% versus females 68.4±10.7%; p=0.619). Patients aged ≥70 years had a significantly lower 28-day survival than younger individuals (≥70 years 41.7±13.5% survival versus <70 years 70.9±6.8% survival; p=0.018 log-rank).
Conclusion: These cases suggest that pneumothorax is a complication of COVID-19. Pneumothorax does not seem to be an independent marker of poor prognosis and we encourage continuation of active treatment where clinically possible.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: A.W. Martinelli has nothing to disclose. Conflict of interest: T. Ingle has nothing to disclose. Conflict of interest: J. Newman has nothing to disclose. Conflict of interest: I. Nadeem has nothing to disclose. Conflict of interest: K. Jackson has nothing to disclose. Conflict of interest: N.D. Lane reports non-financial support from Chiesi, outside the submitted work. Conflict of interest: J. Melhorn has nothing to disclose. Conflict of interest: H.E. Davies has nothing to disclose. Conflict of interest: A.J. Rostron has nothing to disclose. Conflict of interest: A. Adeni has nothing to disclose. Conflict of interest: K. Conroy has nothing to disclose. Conflict of interest: N. Woznitza reports grants from Cancer Research UK and Roy Castle Lung Cancer Foundation, and personal fees from InHealth, outside the submitted work. Conflict of interest: M. Matson has nothing to disclose. Conflict of interest: S.E. Brill has nothing to disclose. Conflict of interest: J. Murray has nothing to disclose. Conflict of interest: A. Shah has nothing to disclose. Conflict of interest: R. Naran has nothing to disclose. Conflict of interest: S.S. Hare has nothing to disclose. Conflict of interest: O. Collas has nothing to disclose. Conflict of interest: S. Bigham has nothing to disclose. Conflict of interest: M. Spiro has nothing to disclose. Conflict of interest: M.M. Huang has nothing to disclose. Conflict of interest: B. Iqbal has nothing to disclose. Conflict of interest: S. Trenfield has nothing to disclose. Conflict of interest: S. Ledot has nothing to disclose. Conflict of interest: S. Desai has nothing to disclose. Conflict of interest: L. Standing has nothing to disclose. Conflict of interest: J. Babar has nothing to disclose. Conflict of interest: R. Mahroof has nothing to disclose. Conflict of interest: I. Smith has nothing to disclose. Conflict of interest: K. Lee has nothing to disclose. Conflict of interest: N. Tchrakain Nothing to declare. Conflict of interest: S. Uys has nothing to disclose. Conflict of interest: W. Ricketts has nothing to disclose. Conflict of interest: A.R.C. Patel has nothing to disclose. Conflict of interest: A. Aujayeb has nothing to disclose. Conflict of interest: M. Kokosi has nothing to disclose. Conflict of interest: A.J.K. Wilkinson has nothing to disclose. Conflict of interest: S.J. Marciniak has nothing to disclose.
Figures
Comment in
-
Pleural diseases and COVID-19: ubi fumus, ibi ignis.Eur Respir J. 2020 Nov 19;56(5):2003308. doi: 10.1183/13993003.03308-2020. Print 2020 Nov. Eur Respir J. 2020. PMID: 32943411 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical