

Prevalence and access to care for cardiovascular risk factors in older people in Sierra Leone: a cross-sectional survey
- PMID: 32907906
- PMCID: PMC7482482
- DOI: 10.1136/bmjopen-2020-038520
Prevalence and access to care for cardiovascular risk factors in older people in Sierra Leone: a cross-sectional survey
Abstract
Introduction: Prevalence of cardiovascular disease risk factors (CVDRFs) is increasing, especially in low-income countries. In Sierra Leone, there is limited empirical data on the prevalence of CVDRFs, and there are no previous studies on the access to care for these conditions.
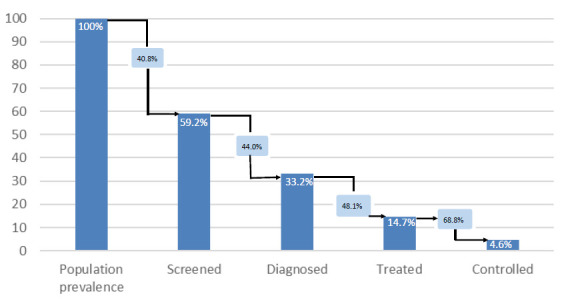
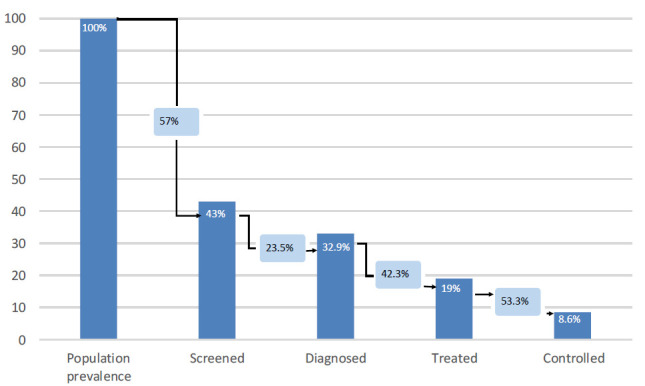
Methods: This study in rural and urban Sierra Leone collected demographic, anthropometric measurements and clinical data from randomly sampled individuals over 40 years old using a household survey. We describe the prevalence of the following risk factors: diabetes, hypertension, dyslipidaemia, overweight or obesity, smoking and having at least one of these risk factors. Cascades of care were constructed for diabetes and hypertension using % of the population with the disease who had previously been tested ('screened'), knew of their condition ('diagnosed'), were on treatment ('treated') or were controlled to target ('controlled'). Multivariable regression was used to test associations between prevalence of CVDRFs and progress through the cascade for hypertension with demographic and socioeconomic variables. In those with recognised disease who did not seek care, reasons for not accessing care were recorded.
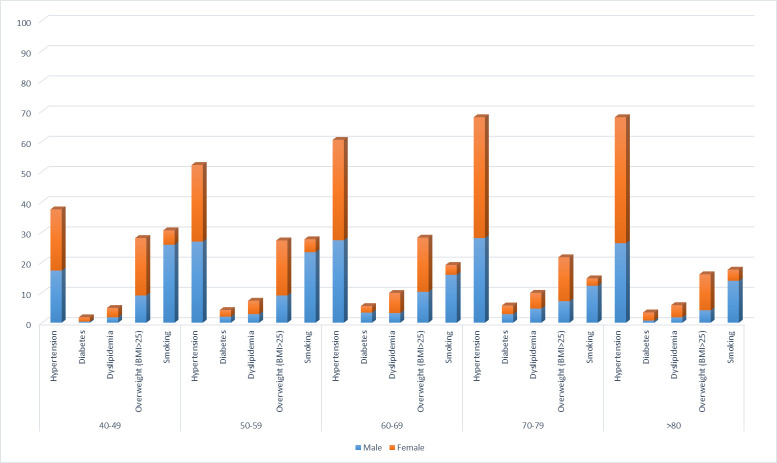
Results: Of 2071 people, 49.6% (95% CI 49.3% to 50.0%) of the population had hypertension, 3.5% (3.4% to 3.6%) had diabetes, 6.7% (6.5% to 7.0%) had dyslipidaemia, 25.6% (25.4% to 25.9%) smoked and 26.5% (26.3% to 26.8%) were overweight/obese; a total of 77.1% (76.6% to 77.5%) had at least one CVDRF. People in urban areas were more likely to have diabetes and be overweight than those living in rural areas. Moreover, being female, more educated or wealthier increased the risk of having all CVDRFs except for smoking. There is a substantial loss of patients at each step of the care cascade for both diabetes and hypertension, with less than 10% of the total population with the conditions being screened, diagnosed, treated and controlled. The most common reasons for not seeking care were lack of knowledge and cost.
Conclusions: In Sierra Leone, CVDRFs are prevalent and access to care is low. Health system strengthening with a focus on increased access to quality care for CVDRFs is urgently needed.
Keywords: epidemiology; health policy; organisation of health services; public health; quality in health care.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- GBD 2017 Causes of Death Collaborators Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the global burden of disease study 2017. Lancet 2018;392:1736–88. 10.1016/S0140-6736(18)32203-7 - DOI - PMC - PubMed
-
- The World Bank Sierra Leone, 2019. Available: https://data.worldbank.org
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources