

Functional Analysis of Rare Genetic Variants in Complement Factor I (CFI) using a Serum-Based Assay in Advanced Age-related Macular Degeneration
- PMID: 32908800
- PMCID: PMC7453046
- DOI: 10.1167/tvst.9.9.37
Functional Analysis of Rare Genetic Variants in Complement Factor I (CFI) using a Serum-Based Assay in Advanced Age-related Macular Degeneration
Abstract
Purpose: Factor I (FI) is a serine protease regulator of the complement system. Genetic variants in CFI are associated with advanced age-related macular degeneration (AAMD). However, the clinical and functional impact of these variants is unknown. This study assessed the functional significance of rare CFI variants using a serum-based assay.
Methods: Carriers of rare variants with (n = 78) and without AAMD (n = 28), and noncarriers with (n = 49) and without AMD (n = 44) were evaluated. Function of FI was determined by measuring the proteolytic cleavage of C3b to iC3b, using the cofactor protein, Factor H.
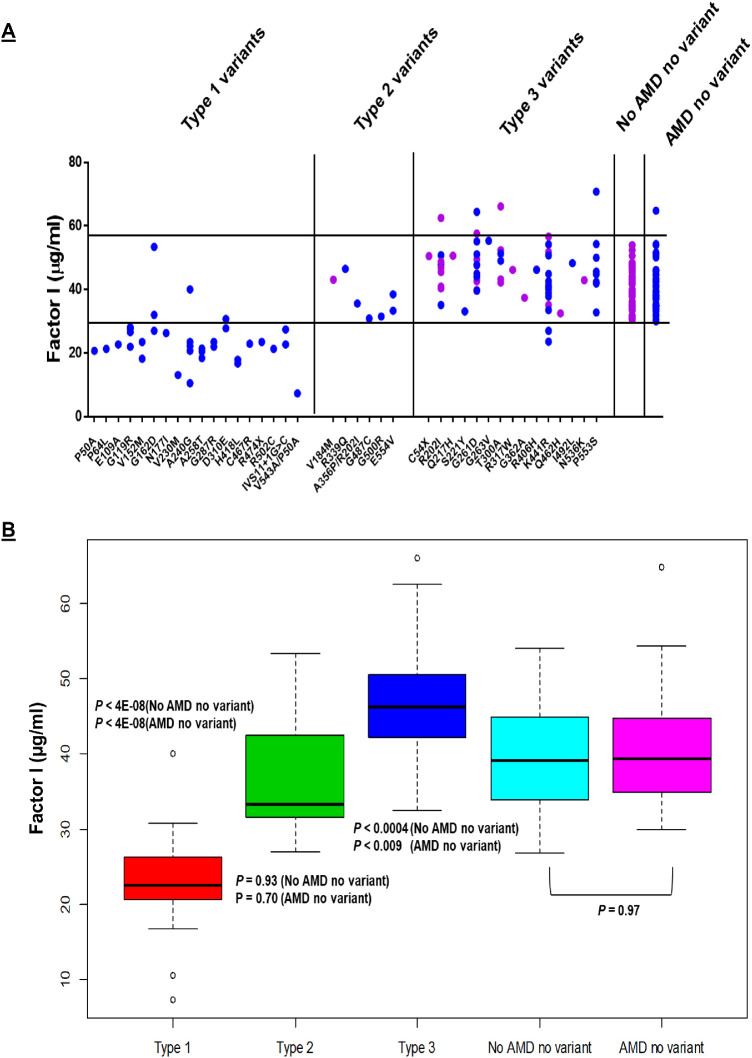
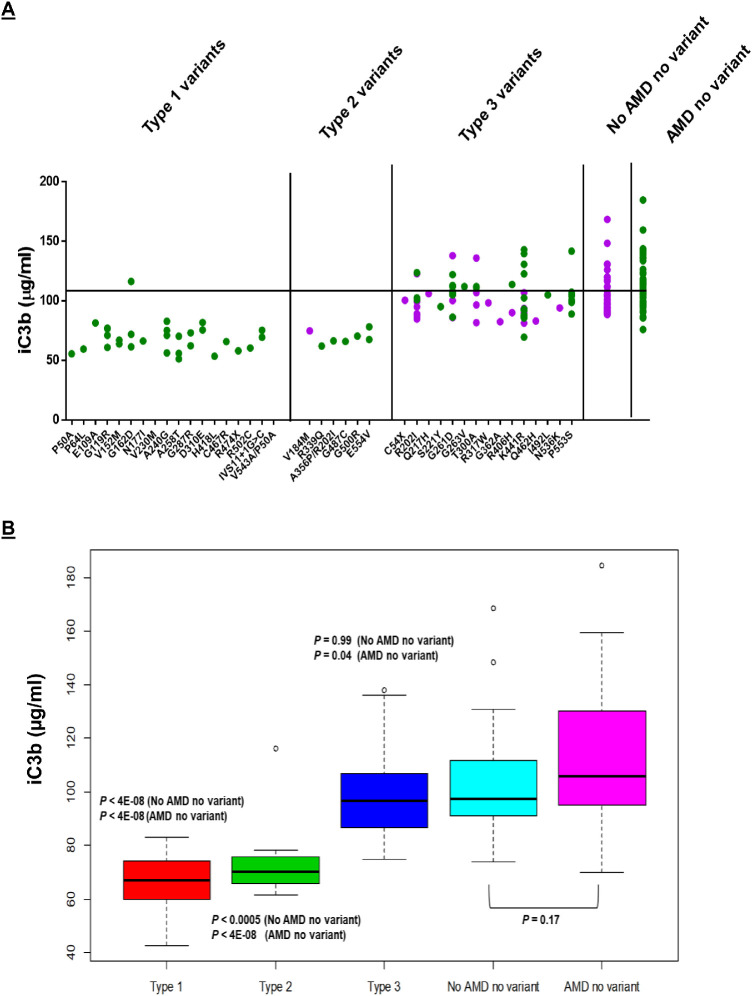
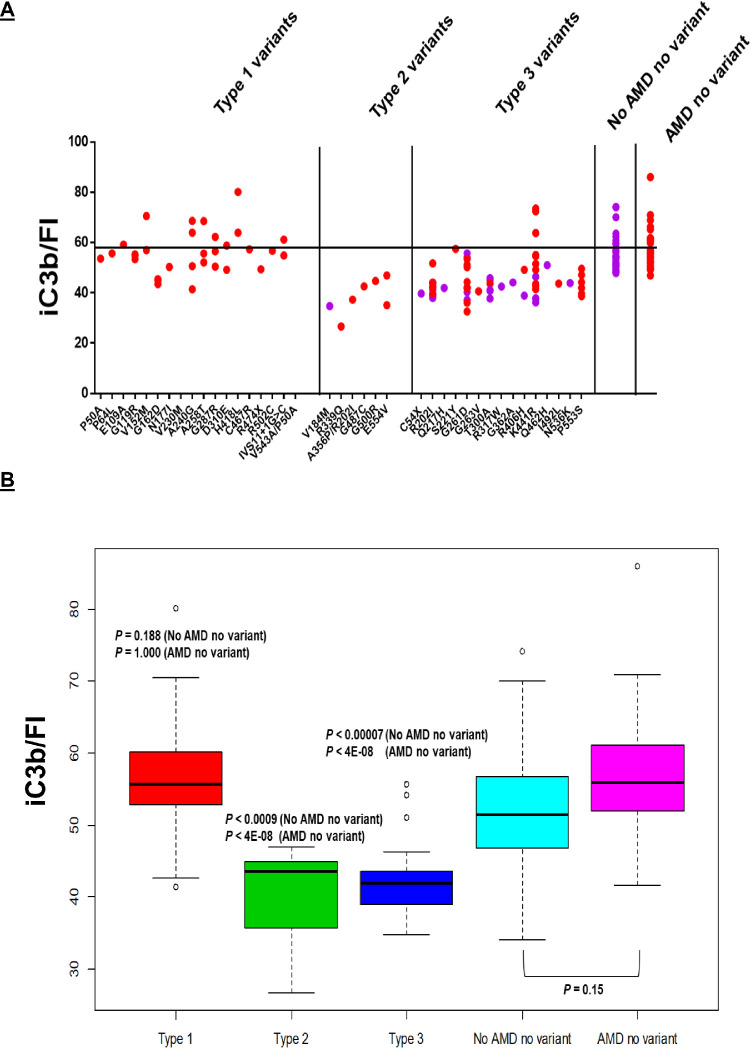
Results: CFI variants were categorized into three groups based on antigenic and functional assessments. Type 1 variants (n = 18) in 35 patients with AAMD demonstrated low serum FI levels and a corresponding decrease in FI function. Type 2 variants (n = 6) in 7 individuals demonstrated normal serum FI antigenic levels but reduced degradation of C3b to iC3b. Type 3 variants (n = 15) in 64 individuals demonstrated normal antigenic levels and degradation of C3b to iC3b. However, iC3b generation was low when measured per unit of FI. Thus most rare CFI variants demonstrate either low antigenic levels (type 1) or normal levels but reduced function (types 2 or 3).
Conclusions: Results provide for the first time a comprehensive functional assessment in serum of CFI rare genetic variants and further establish FI's key role in the pathogenesis of AAMD.
Translational relevance: Stratifying patients in the clinic with a rare CFI variant will facilitate screening and targeting patients most likely to benefit from complement therapies.
Keywords: Factor I; age-related macular degeneration; complement; functional analysis; rare genetic variants.
Copyright 2020 The Authors.
Conflict of interest statement
Disclosures: A. Java, Alexion Pharmaceuticals (C), Gemini Therapeutics (C), Novartis Pharmaceuticals (C); P. Baciu, Allergan (E); R. Widjajahakim, None; Y.J. Sung, None; J. Yang, Allergan (E); D. Kavanagh, Gyroscope Therapeutics (S), Alexion Pharmaceuticals (C), Sarepta (C), Actelion (C), Novartis (C), Apellis (C); J. Atkinson, Compliment Corporation (I), Kypha (I,C), Gemini Therapeutics (I), Q32BIO INC - formerly AdMiRx (I,C), Celldex Therapeutics (C), Clinical Pharmacy Services (C), Achillion Pharmaceuticals (C), BioMarin Pharmaceutical (C), Annexon Biosciences (C); J. Seddon, Laboratoires THEA (C), Gemini Therapeutics, Inc (F)
Figures
References
-
- Wong WL, Su X, Li X, et al.. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014; 2: e106–e116. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
