

Acetabular Bone Defect in Total Hip Arthroplasty for Crowe II or III Developmental Dysplasia of the Hip: A Finite Element Study
- PMID: 32908892
- PMCID: PMC7468597
- DOI: 10.1155/2020/4809013
Acetabular Bone Defect in Total Hip Arthroplasty for Crowe II or III Developmental Dysplasia of the Hip: A Finite Element Study
Abstract
Background: The purpose of this study was to establish the finite element analysis (FEA) model of acetabular bone defect in Crowe type II or III developmental dysplasia of the hip (DDH), which could evaluate the stability of the acetabular cup with different types of bone defects, different diameters of femoral ceramic heads, and the use of screws and analyze the stress distribution of screws.
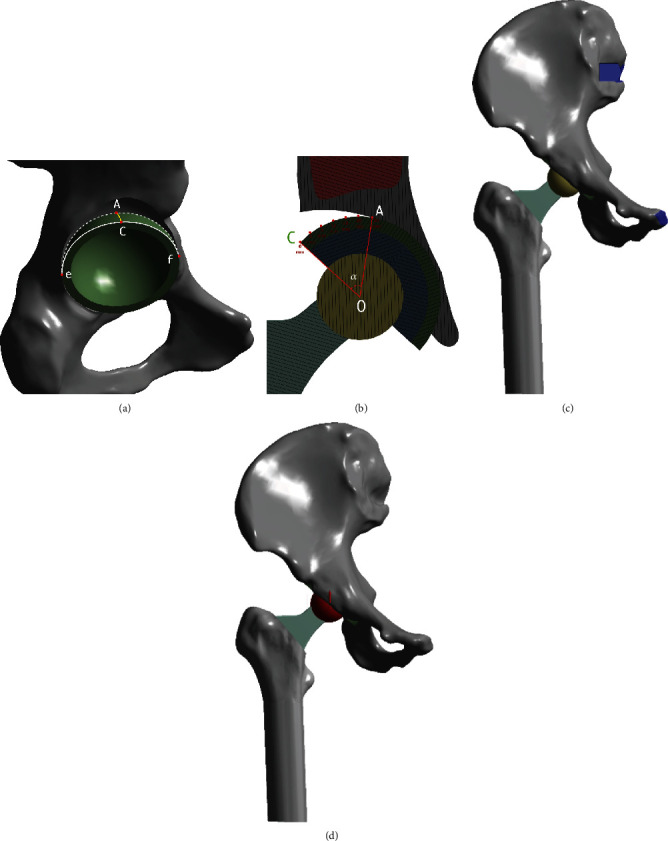
Methods: The FEA model was based on the CT scan of a female patient without any acetabular bone defect. The model of acetabular bone defect in total hip arthroplasty for Crowe II or III DDH was made by the increasing superolateral bone defect area of the acetabular cup. Point A was located in the most medial part of the acetabular bone defect. A 52 mm PINNACLE cup with POROCOAT Porous coating was implanted, and two screws (the lengths were 25 mm and 40 mm) were implanted to fix the acetabular cup. The stability of the acetabular cup and the von Mises stress of point A and screws were analyzed by a single-legged stance loading applied in 1948 N (normal working). The different diameters of the femoral ceramic head (28 mm, 32 mm, and 36 mm) were also analyzed.
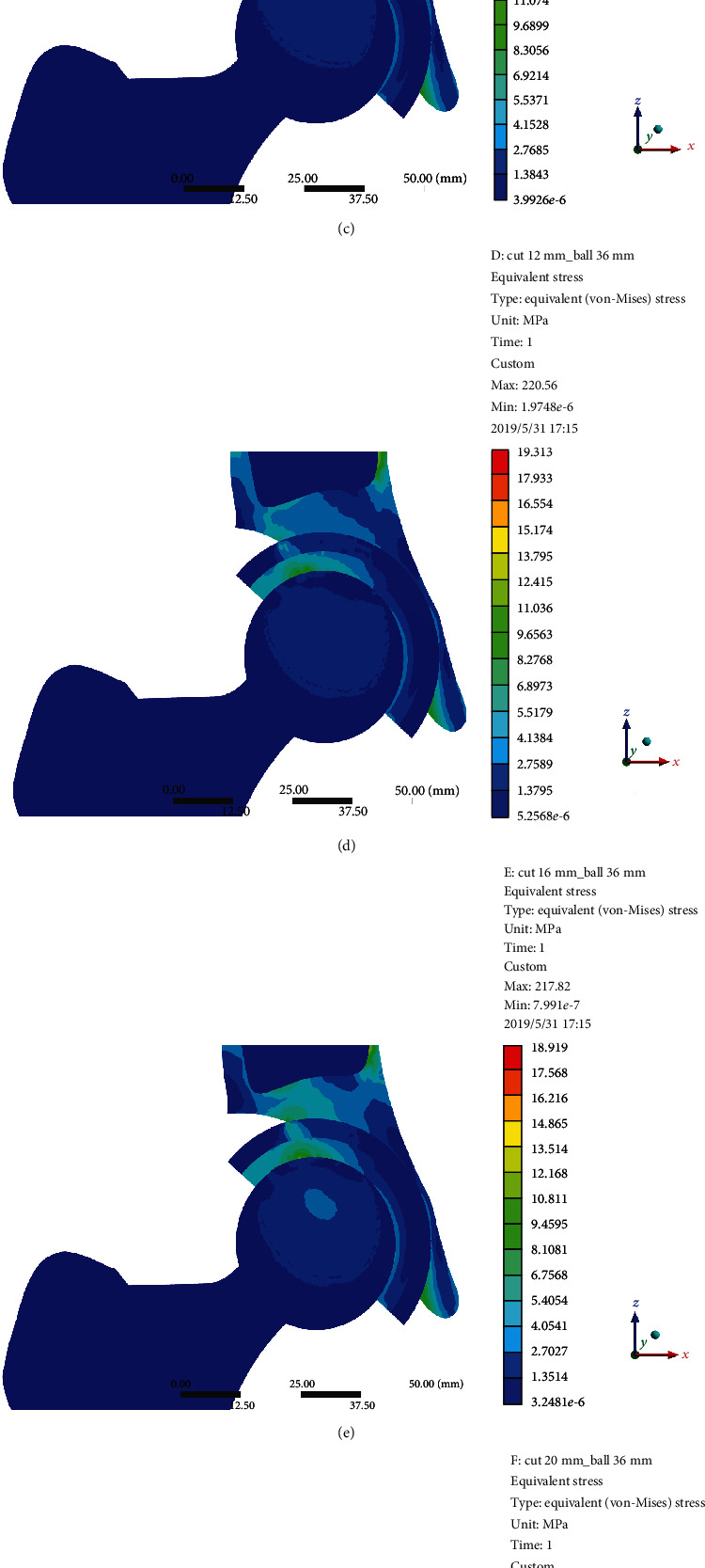
Results: The von Mises stress of point A was gradually increased with the increasing uncoverage values. When the uncoverage values exceeded 24.5%, the von Mises stress of point A without screws increased significantly, leading to instability of the cup. Screws could effectively reduce the von Mises stress of point A with uncoverage values of more than 24.5%. However, the peak von Mises stress in the screws with the uncoverage values that exceeded 24.5% was considerably increased. The diameter of the femoral ceramic head had no significant effect on the von Mises stress and the stability of the acetabular cup.
Conclusions: We recommend that uncoverage values of less than 24.5% with or without screw is safe for patients with Crowe II or III DDH.
Copyright © 2020 Yinqiao Du et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures


Similar articles
-
The press-fit technique without screws and bone graft can be used as an alternative method in Crowe type II and III hip dysplasia.Turk J Med Sci. 2023 Aug 11;53(5):1448-1457. doi: 10.55730/1300-0144.5712. eCollection 2023. Turk J Med Sci. 2023. PMID: 38813005 Free PMC article.
-
[Hip joint biomechanical analysis of the acetabular anatomical reconstruction and nonanatomical reconstruction in total hip arthroplasty for Crowe type Ⅲ developmental dysplasia of the hip by finite element method].Zhongguo Gu Shang. 2024 May 25;37(5):505-15. doi: 10.12200/j.issn.1003-0034.20221143. Zhongguo Gu Shang. 2024. PMID: 38778536 Chinese.
-
[Biomechanical research progress of common acetabular reconstruction techniques for Crowe type Ⅱ and Ⅲ developmental dysplasia of the hip].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023 Mar 15;37(3):353-359. doi: 10.7507/1002-1892.202211052. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023. PMID: 36940996 Free PMC article. Chinese.
-
[Advances in revision surgery after primary total hip arthroplasty for Crowe type Ⅳ developmental dysplasia of the hip].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023 Dec 15;37(12):1548-1555. doi: 10.7507/1002-1892.202309016. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023. PMID: 38130200 Free PMC article. Review. Chinese.
-
Total Hip Arthroplasty in Patients with Crowe III/IV Developmental Dysplasia of the Hip: Acetabular Morphology and Reconstruction Techniques.Orthop Surg. 2023 Jun;15(6):1468-1476. doi: 10.1111/os.13733. Epub 2023 Apr 28. Orthop Surg. 2023. PMID: 37114450 Free PMC article. Review.
Cited by
-
Biomechanical analysis and clinical observation of 3D-printed acetabular prosthesis for the acetabular reconstruction of total hip arthroplasty in Crowe III hip dysplasia.Front Bioeng Biotechnol. 2023 Sep 15;11:1219745. doi: 10.3389/fbioe.2023.1219745. eCollection 2023. Front Bioeng Biotechnol. 2023. PMID: 37790252 Free PMC article.
-
The application of additive manufacturing technology in pelvic surgery: A bibliometrics analysis.Front Bioeng Biotechnol. 2023 Apr 6;11:1123459. doi: 10.3389/fbioe.2023.1123459. eCollection 2023. Front Bioeng Biotechnol. 2023. PMID: 37091335 Free PMC article.
-
Mid-term outcomes after total hip arthroplasty in 106 Crowe II/III hips: different hip center positions.Eur J Med Res. 2022 Dec 9;27(1):282. doi: 10.1186/s40001-022-00936-0. Eur J Med Res. 2022. PMID: 36494873 Free PMC article.
-
Integrated Acetabular Prosthesis Versus Bone Grafting in Total Hip Arthroplasty for Crowe Type II and III Hip Dysplasia: A Retrospective Case-Control Study.Orthop Surg. 2024 Oct;16(10):2401-2409. doi: 10.1111/os.14143. Epub 2024 Jul 23. Orthop Surg. 2024. PMID: 39043609 Free PMC article.
-
The press-fit technique without screws and bone graft can be used as an alternative method in Crowe type II and III hip dysplasia.Turk J Med Sci. 2023 Aug 11;53(5):1448-1457. doi: 10.55730/1300-0144.5712. eCollection 2023. Turk J Med Sci. 2023. PMID: 38813005 Free PMC article.
References
-
- Hitz O. F., Flecher X., Parratte S., Ollivier M., Argenson J.-N. Minimum 10-year outcome of one-stage total hip arthroplasty without subtrochanteric osteotomy using a cementless custom stem for Crowe III and IV hip dislocation. The Journal of Arthroplasty. 2018;33(7):2197–2202. doi: 10.1016/j.arth.2018.02.055. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
