

doi: 10.1093/noajnl/vdaa076.
eCollection 2020 Jan-Dec.
Cervicomedullary hemangioblastoma treated with bevacizumab
Affiliations
- PMID: 32908970
- PMCID: PMC7470470
- DOI: 10.1093/noajnl/vdaa076
Item in Clipboard
Cervicomedullary hemangioblastoma treated with bevacizumab
Neurooncol Adv.
.
No abstract available
Keywords: bevacizumab; hemangioblastoma.
Figures
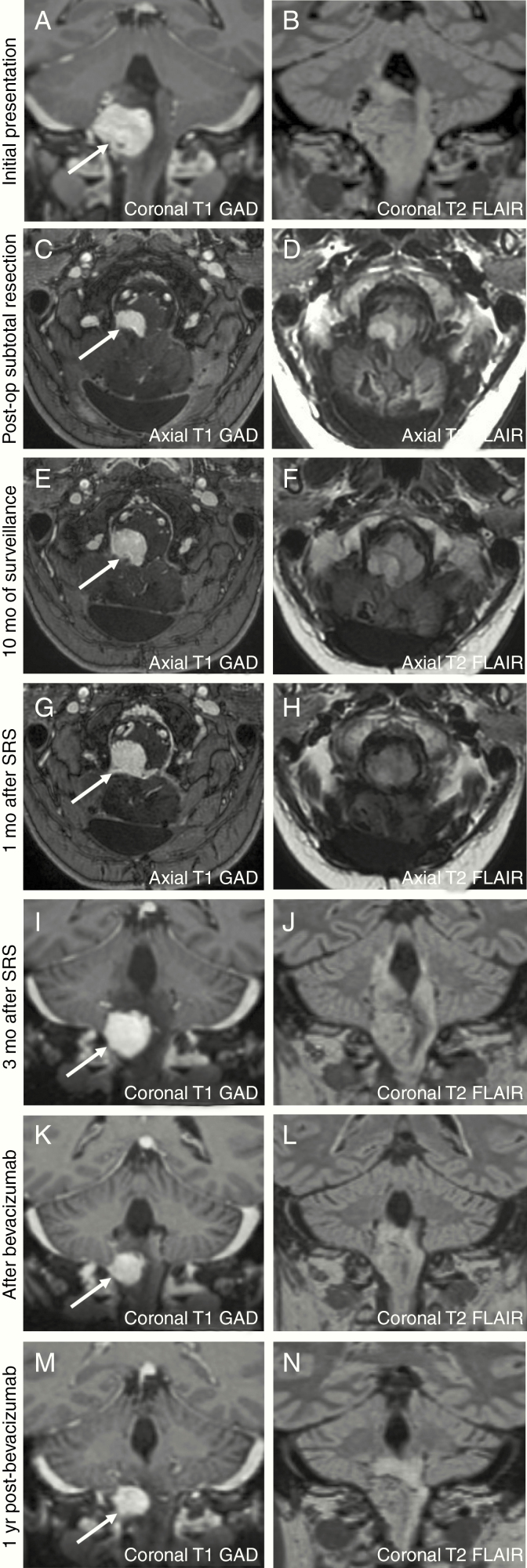
At the initial presentation, MRI revealed a mass at the cervicomedullary junction measuring 2 × 2.5 × 2.3 cm (A and B). After subtotal surgical resection (C and D), the size of the hemangioblastoma decreased to 1.6 × 0.6 × 1.1 cm. With 10 months of surveillance, the hemangioblastoma increased to 1.6 × 1.0 × 1.4 cm (E and F). There was an enlargement of the hemangioblastoma 1-month (mo) post-stereotactic radiosurgery, measuring 1.9 × 1.5 × 1.8 cm, with associated edema and hydrocephalus (G and H). Ongoing surveillance revealed a further increase of the hemangioblastoma (2.0 × 1.8 × 2.0 cm) and increased surrounding edema (I and J). After bevacizumab therapy, there was a decrease in the size of the hemangioblastoma, measuring 1.4 × 1.5 × 1.7 cm (K and L) and reduction of surrounding edema. Over 1 year of clinical surveillance, the hemangioblastoma has remained stable in size, measuring 1.4 × 1.6 × 1.7 cm (M and N).
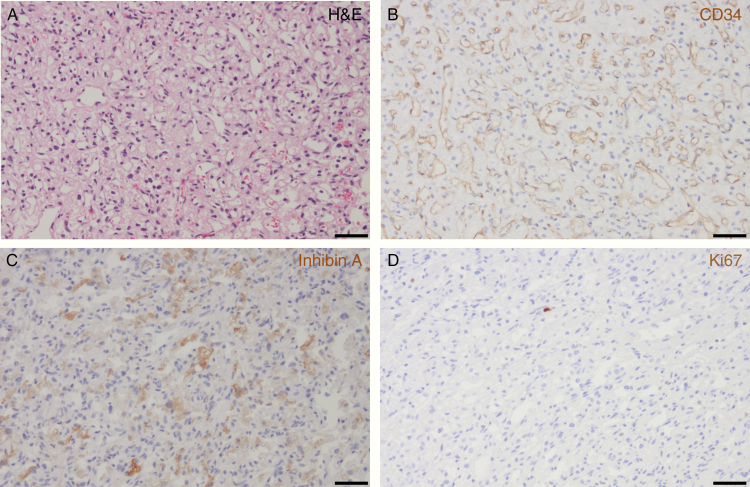
Surgical resection from the cervicomedullary mass shows typical features of hemangioblastoma with numerous irregular small capillary-type vascular channels and an intervening cell population (so-called “stromal” cells) on hematoxylin and eosin (H&E) staining, 200× magnification (A) with the scale bar measuring 50 µm. There are prominent capillary-type vascular spaces highlighted by CD34-positive immunohistochemistry staining for endothelial cells, 200× magnification (B) with the scale bar measuring 50 µm. The non-vascular tumor cells (“stromal” cells) exhibit characteristic inhibin A positivity by immunohistochemistry, 200× magnification (C) with the scale bar measuring 50 µm. There is a very low proliferative activity of the tumor with only a rare tumor cell nucleus positive for Ki67 on immunohistochemistry, 200× magnification (D) with the scale bar measuring 50 µm.
References
-
- Gläsker S, Klingler JH, Müller K, et al. . Essentials and pitfalls in the treatment of CNS hemangioblastomas and von Hippel-Lindau disease. Cent Eur Neurosurg. 2010;71(2):80–87. - PubMed
-
- Pierscianek DWS, Keyvani K, El Hindy N, et al. . Study of angiogenic signaling pathways in hemangioblastoma. Neuropathology. 2017;37(1):3–11. - PubMed
-
- Kano H, Shuto T, Iwai Y, et al. . Stereotactic radiosurgery for intracranial hemangioblastomas: a retrospective international outcome study. J Neurosurg. 2015;122(6):1469–1478. - PubMed
LinkOut - more resources
Full Text Sources