

This is a preprint.
SARS-CoV-2 Infections Among Children in the Biospecimens from Respiratory Virus-Exposed Kids (BRAVE Kids) Study
- PMID: 32908992
- PMCID: PMC7480040
- DOI: 10.1101/2020.08.18.20166835
SARS-CoV-2 Infections Among Children in the Biospecimens from Respiratory Virus-Exposed Kids (BRAVE Kids) Study
Update in
-
Severe Acute Respiratory Syndrome Coronavirus 2 Infections Among Children in the Biospecimens from Respiratory Virus-Exposed Kids (BRAVE Kids) Study.Clin Infect Dis. 2021 Nov 2;73(9):e2875-e2882. doi: 10.1093/cid/ciaa1693. Clin Infect Dis. 2021. PMID: 33141180 Free PMC article.
Abstract
Background: Children with SARS-CoV-2 infection typically have mild symptoms that do not require medical attention, leaving a gap in our understanding of the spectrum of illnesses that the virus causes in children.
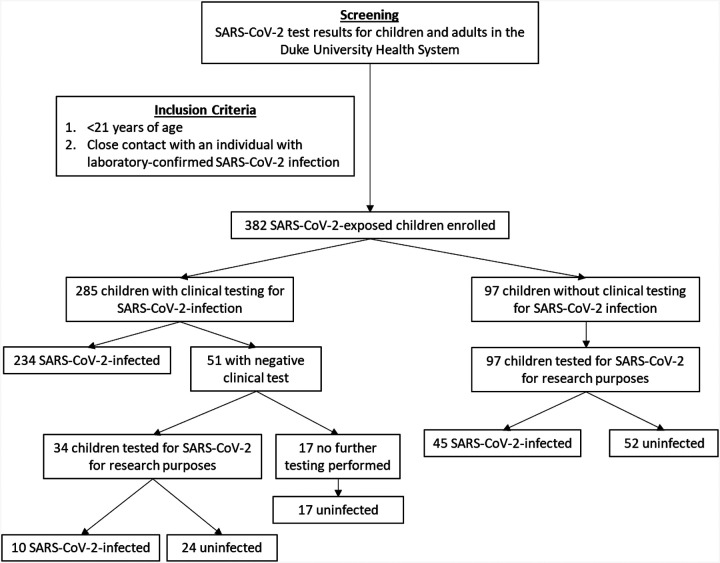
Methods: We conducted a prospective cohort study of children and adolescents (<21 years of age) with a SARS-CoV-2-infected close contact. We collected nasopharyngeal or nasal swabs at enrollment and tested for SARS-CoV-2 using a real-time PCR assay.
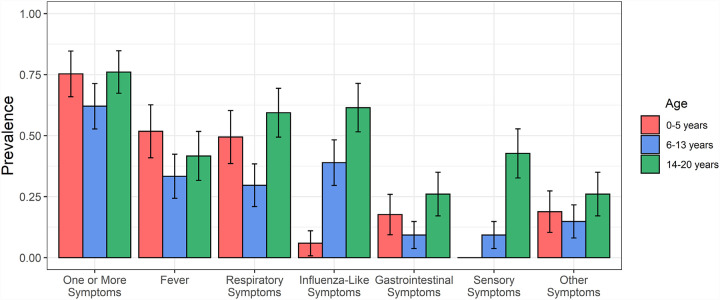
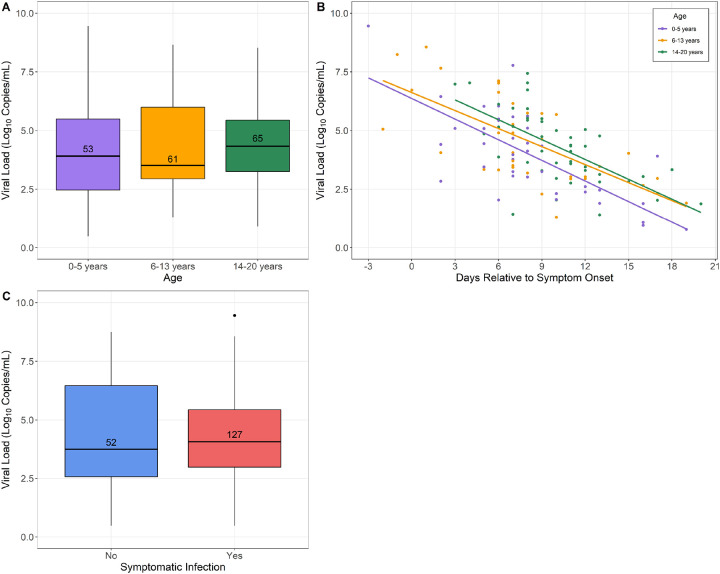
Results: Of 382 children, 289 (76%) were SARS-CoV-2-infected. SARS-CoV-2-infected children were more likely to be Hispanic (p<0.0001), less likely to have a history of asthma (p=0.009), and more likely to have an infected sibling contact (p=0.0007) than uninfected children. Children ages 6-13 years were frequently asymptomatic (38%) and had respiratory symptoms less often than younger children (30% vs. 49%; p=0.008) or adolescents (30% vs. 59%; p<0.0001). Compared to children ages 6-13 years, adolescents more frequently reported influenza-like (61% vs. 39%; p=0.002), gastrointestinal (26% vs. 9%; p=0.003), and sensory symptoms (43% vs. 9%; p<0.0001), and had more prolonged illnesses [median (IQR) duration: 7 (4, 12) vs. 4 (3, 8) days; p=0.004]. Despite the age-related variability in symptoms, we found no differences in nasopharyngeal viral load by age or between symptomatic and asymptomatic children.
Conclusions: Hispanic ethnicity and an infected sibling close contact are associated with increased SARS-CoV-2 infection risk among children, while a history of asthma is associated with decreased risk. Age-related differences in the clinical manifestations of SARS-CoV-2 infection must be considered when evaluating children for COVID-19 and in developing screening strategies for schools and childcare settings.
Conflict of interest statement
Declarations
SRP consults for cytomegalovirus vaccine programs at Merck, Sanofi, Moderna, and Pfizer, and receives support for research from Moderna and Merck. EBW is an investigator for clinical trials funded by Pfizer and Moderna. All other authors have no conflicts of interest to declare.
Figures
References
-
- Davies NG, Klepac P, Liu Y, Prem K, Jit M, Pearson CAB, et al. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nature medicine. 2020. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous