

Bone Development in Transgender Adolescents Treated With GnRH Analogues and Subsequent Gender-Affirming Hormones
- PMID: 32909025
- PMCID: PMC7524308
- DOI: 10.1210/clinem/dgaa604
Bone Development in Transgender Adolescents Treated With GnRH Analogues and Subsequent Gender-Affirming Hormones
Abstract
Context: Hormonal interventions in adolescents with gender dysphoria may have adverse effects, such as reduced bone mineral accrual.
Objective: To describe bone mass development in adolescents with gender dysphoria treated with gonadotropin-releasing hormone analogues (GnRHa), subsequently combined with gender-affirming hormones.
Design: Observational prospective study.
Subjects: 51 transgirls and 70 transboys receiving GnRHa and 36 transgirls and 42 transboys receiving GnRHa and gender-affirming hormones, subdivided into early- and late-pubertal groups.
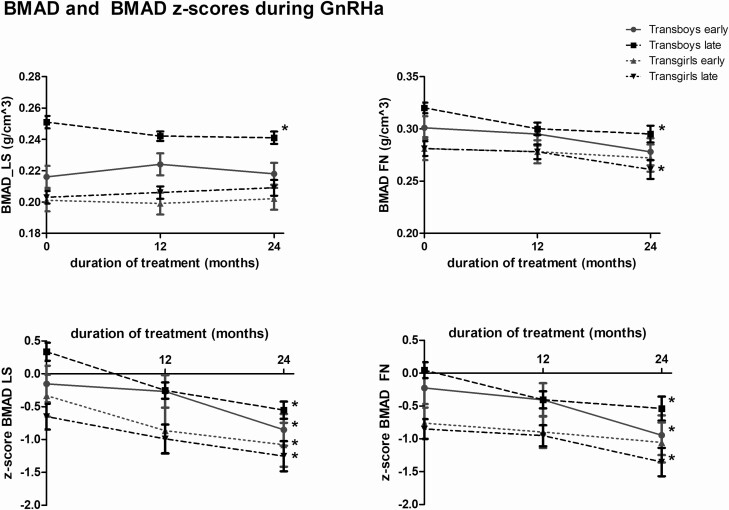
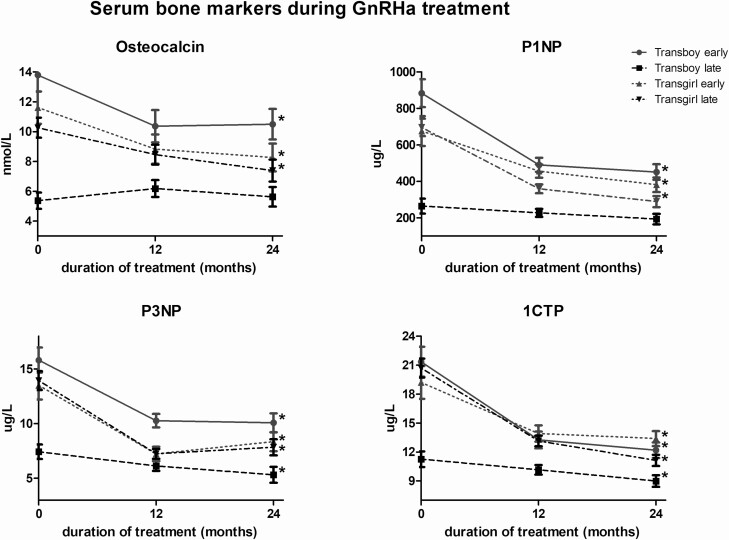
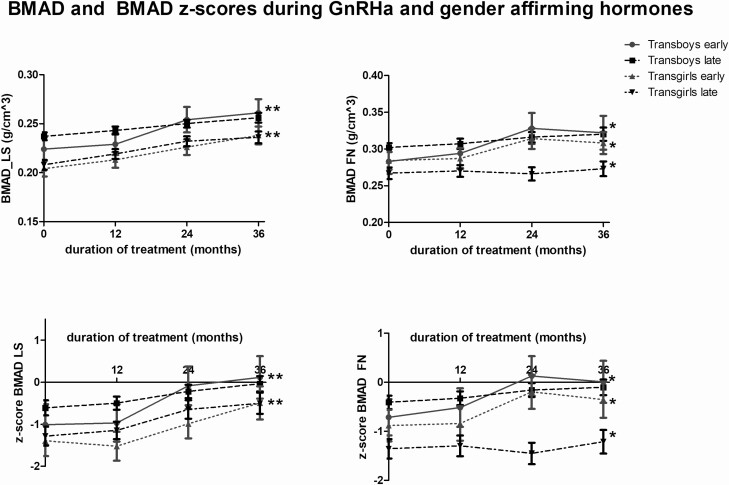
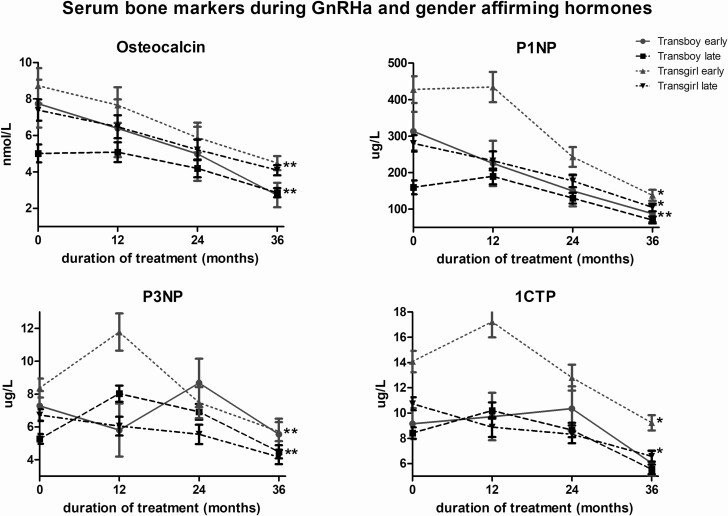
Main outcome measures: Bone mineral apparent density (BMAD), age- and sex-specific BMAD z-scores, and serum bone markers.
Results: At the start of GnRHa treatment, mean areal bone mineral density (aBMD) and BMAD values were within the normal range in all groups. In transgirls, the mean z-scores were well below the population mean. During 2 years of GnRHa treatment, BMAD stabilized or showed a small decrease, whereas z-scores decreased in all groups. During 3 years of combined administration of GnRHa and gender-affirming hormones, a significant increase of BMAD was found. Z-scores normalized in transboys but remained below zero in transgirls. In transgirls and early pubertal transboys, all bone markers decreased during GnRHa treatment.
Conclusions: BMAD z-scores decreased during GnRHa treatment and increased during gender-affirming hormone treatment. Transboys had normal z-scores at baseline and at the end of the study. However, transgirls had relatively low z-scores, both at baseline and after 3 years of estrogen treatment. It is currently unclear whether this results in adverse outcomes, such as increased fracture risk, in transgirls as they grow older.
Keywords: GnRH analogue; adolescents; bone; bone mineral density; gender dysphoria; sex steroids; transgender.
© Endocrine Society 2020.
Figures
Similar articles
-
Puberty suppression in adolescents with gender dysphoria: an emerging issue with multiple implications.Front Endocrinol (Lausanne). 2024 Jun 14;15:1309904. doi: 10.3389/fendo.2024.1309904. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38988996 Free PMC article. Review.
-
Changes in Adrenal Androgens During Puberty Suppression and Gender-Affirming Hormone Treatment in Adolescents With Gender Dysphoria.J Sex Med. 2018 Sep;15(9):1357-1363. doi: 10.1016/j.jsxm.2018.07.017. J Sex Med. 2018. PMID: 30224022
-
The effect of GnRH analogue treatment on bone mineral density in young adolescents with gender dysphoria: findings from a large national cohort.J Pediatr Endocrinol Metab. 2019 Oct 25;32(10):1077-1081. doi: 10.1515/jpem-2019-0046. J Pediatr Endocrinol Metab. 2019. PMID: 31472062 Clinical Trial.
-
Bone mass in young adulthood following gonadotropin-releasing hormone analog treatment and cross-sex hormone treatment in adolescents with gender dysphoria.J Clin Endocrinol Metab. 2015 Feb;100(2):E270-5. doi: 10.1210/jc.2014-2439. Epub 2014 Nov 26. J Clin Endocrinol Metab. 2015. PMID: 25427144
-
Adolescents with gender dysphoria.Best Pract Res Clin Endocrinol Metab. 2015 Jun;29(3):485-95. doi: 10.1016/j.beem.2015.01.004. Epub 2015 Jan 24. Best Pract Res Clin Endocrinol Metab. 2015. PMID: 26051304 Review.
Cited by
-
Puberty suppression in adolescents with gender dysphoria: an emerging issue with multiple implications.Front Endocrinol (Lausanne). 2024 Jun 14;15:1309904. doi: 10.3389/fendo.2024.1309904. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38988996 Free PMC article. Review.
-
Misgendering a transgender woman using FORDISC 3.1: A case study.Forensic Sci Int Synerg. 2023 Jun 18;7:100342. doi: 10.1016/j.fsisyn.2023.100342. eCollection 2023. Forensic Sci Int Synerg. 2023. PMID: 37415608 Free PMC article.
-
Update on bioethical, medical and fertility issues in gender incongruence during transition age.J Endocrinol Invest. 2023 Sep;46(9):1725-1736. doi: 10.1007/s40618-023-02077-5. Epub 2023 Apr 18. J Endocrinol Invest. 2023. PMID: 37071372 Free PMC article. Review.
-
Gender-Affirming Care of Transgender and Gender-Diverse Youth: Current Concepts.Annu Rev Med. 2023 Jan 27;74:107-116. doi: 10.1146/annurev-med-043021-032007. Epub 2022 Oct 19. Annu Rev Med. 2023. PMID: 36260812 Free PMC article. Review.
-
Cardiovascular Risk Associated With Gender Affirming Hormone Therapy in Transgender Population.Front Endocrinol (Lausanne). 2021 Sep 30;12:718200. doi: 10.3389/fendo.2021.718200. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34659112 Free PMC article. Review.
References
-
- Skordis N, Butler G, de Vries MC, Main K, Hannema SE. ESPE and PES international survey of centers and clinicians delivering specialist care for children and adolescents with gender dysphoria. Horm Res Paediatr. 2018;90(5):326-331. - PubMed
-
- Wiepjes CM, Nota NM, de Blok CJM, et al. The Amsterdam Cohort of gender dysphoria study (1972–2015): trends in prevalence, treatment, and regrets. J Sex Med. 2018;15:582–90. - PubMed
-
- Hembree WC, Cohen-Kettenis PT, Gooren L, et al. Endocrine treatment of gender-dysphoric/gender-incongruent persons: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2017;102(11):3869-3903. - PubMed
-
- Waal HAD-vd, Cohen-Kettenis PT. Clinical management of gender identity disorder in adolescents: a protocol on psychological and paediatric endocrinology aspects. Eur J Endocrinol. 2006;155:S131.
-
- Magarey AM, Boulton TJ, Chatterton BE, Schultz C, Nordin BE, Cockington RA. Bone growth from 11 to 17 years: relationship to growth, gender and changes with pubertal status including timing of menarche. Acta Paediatr. 1999;88(2):139-146. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
