

Motion analysis for better understanding of psychomotor skills in laparoscopy: objective assessment-based simulation training using animal organs
- PMID: 32909201
- PMCID: PMC8263434
- DOI: 10.1007/s00464-020-07940-7
Motion analysis for better understanding of psychomotor skills in laparoscopy: objective assessment-based simulation training using animal organs
Erratum in
-
Correction to: Motion analysis for better understanding of psychomotor skills in laparoscopy: objective assessment-based simulation training using animal organs.Surg Endosc. 2021 Aug;35(8):4417. doi: 10.1007/s00464-020-08038-w. Surg Endosc. 2021. PMID: 32995966 Free PMC article. No abstract available.
Abstract
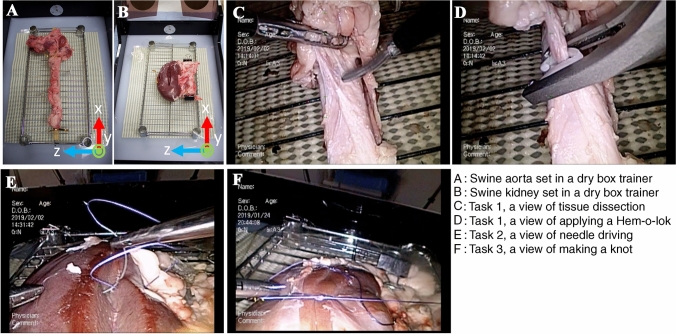
Background: Our aim was to characterize the motions of multiple laparoscopic surgical instruments among participants with different levels of surgical experience in a series of wet-lab training drills, in which participants need to perform a range of surgical procedures including grasping tissue, tissue traction and dissection, applying a Hem-o-lok clip, and suturing/knotting, and digitize the level of surgical competency.
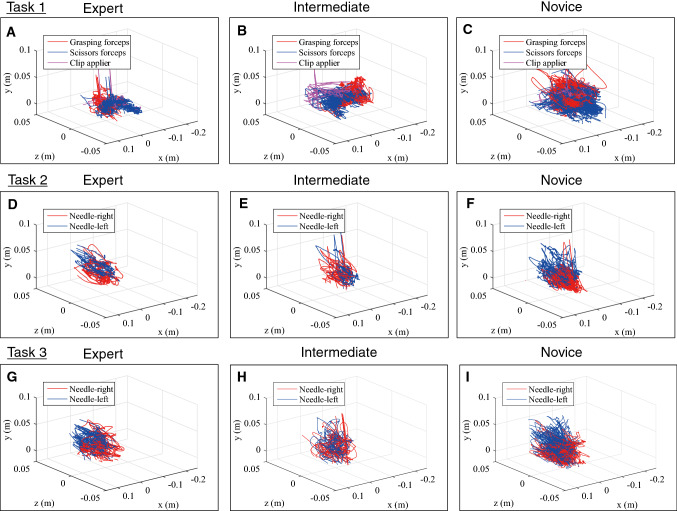
Methods: Participants performed tissue dissection around the aorta, dividing encountered vessels after applying a Hem-o-lok (Task 1), and renal parenchymal closure (Task 2: suturing, Task 3: suturing and knot-tying), using swine cadaveric organs placed in a box trainer under a motion capture (Mocap) system. Motion-related metrics were compared according to participants' level of surgical experience (experts: 50 ≤ laparoscopic surgeries, intermediates: 10-49, novices: 0-9), using the Kruskal-Wallis test, and significant metrics were subjected to principal component analysis (PCA).
Results: A total of 15 experts, 12 intermediates, and 18 novices participated in the training. In Task 1, a shorter path length and faster velocity/acceleration/jerk were observed using both scissors and a Hem-o-lok applier in the experts, and Hem-o-lok-related metrics markedly contributed to the 1st principal component on PCA analysis, followed by scissors-related metrics. Higher-level skills including a shorter path length and faster velocity were observed in both hands of the experts also in tasks 2 and 3. Sub-analysis showed that, in experts with 100 ≤ cases, scissors moved more frequently in the "close zone (0 ≤ to < 2.0 cm from aorta)" than those with 50-99 cases.
Conclusion: Our novel Mocap system recognized significant differences in several metrics in multiple instruments according to the level of surgical experience. "Applying a Hem-o-lok clip on a pedicle" strongly reflected the level of surgical experience, and zone-metrics may be a promising tool to assess surgical expertise. Our next challenge is to give completely objective feedback to trainees on-site in the wet-lab.
Keywords: Laparoscopic surgery; Motion capture; Simulation training; Surgical education.
Conflict of interest statement
Koki Ebina, Takashige Abe, Madoka Higuchi, Jun Furumido, Naoya Iwahara, Masafumi Kon, Kiyohiko Hotta, Shunsuke Komizunai, Yo Kurashima, Hiroshi Kikuchi, Ryuji Matsumoto, Takahiro Osawa, Sachiyo Murai, Teppei Tsujita, Kazuya Sase, Xiaoshuai Chen, Atsushi Konno and Nobuo Shinohara have no conflicts of interest or financial ties to disclose.
Figures





References
-
- Higuchi M, Abe T, Hotta K, Morita K, Miyata H, Furumido J, Iwahara N, Kon M, Osawa T, Matsumoto R, Kikuchi H, Kurashima Y, Murai S, Aydin A, Raison N, Ahmed K, Khan MS, Dasgupta P, Shinohara N (2020) Development and validation of a porcine organ model for training in essential laparoscopic surgical skills. Int J Urol. 10.1111/iju.14315 - PMC - PubMed
-
- Moorthy K, Munz Y, Dosis A, Bello F, Chang A, Darzi A. Bimodal assessment of laparoscopic suturing skills: construct and concurrent validity. Surg Endosc. 2004;18:1608–1612. - PubMed
-
- Egi H, Okajima M, Yoshimitsu M, Ikeda S, Miyata Y, Masugami H, Kawahara T, Kurita Y, Kaneko M, Asahara T. Objective assessment of endoscopic surgical skills by analyzing direction-dependent dexterity using the Hiroshima University Endoscopic Surgical Assessment Device (HUESAD) Surg Today. 2008;38:705–710. doi: 10.1007/s00595-007-3696-0. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
