

Modulation of Cardiometabolic Disease Markers by Type I Interferon Inhibition in Systemic Lupus Erythematosus
- PMID: 32909675
- PMCID: PMC11302498
- DOI: 10.1002/art.41518
Modulation of Cardiometabolic Disease Markers by Type I Interferon Inhibition in Systemic Lupus Erythematosus
Abstract
Objective: Neutrophil dysregulation and the type I interferon (IFN) axis have been proposed to contribute to premature cardiovascular disease, a leading cause of mortality in patients with systemic lupus erythematosus (SLE). In the present study, we evaluated the ability of anifrolumab, a type I IFN receptor-blocking antibody, to reduce neutrophil extracellular trap (NET) formation and modulate cardiometabolic disease markers in comparison to placebo.
Methods: Study subjects comprised patients with moderate-to-severe SLE who were enrolled in phase IIb of the MUSE trial (A Phase II, Randomized Study to Evaluate the Efficacy and Safety of MEDI-546 in Subjects with Systemic Lupus Erythematosus), with healthy individuals as controls. Blood samples were collected from SLE patients (n = 305) and healthy controls (n = 10-20) before the initiation of treatment (baseline) and from SLE patients after they had been treated with 300 mg of anifrolumab (n = 99) or placebo (n = 102). Baseline IFN gene signature test status was determined, and the IFN gene signature (21-gene panel) was monitored over time. Serum proteins were measured by multiplex immunoassay or ultrasensitive Simoa assay. NET complexes, cholesterol efflux capacity (CEC), and glycoprotein acetylation (GlycA) and other lipid parameters were assessed in plasma.
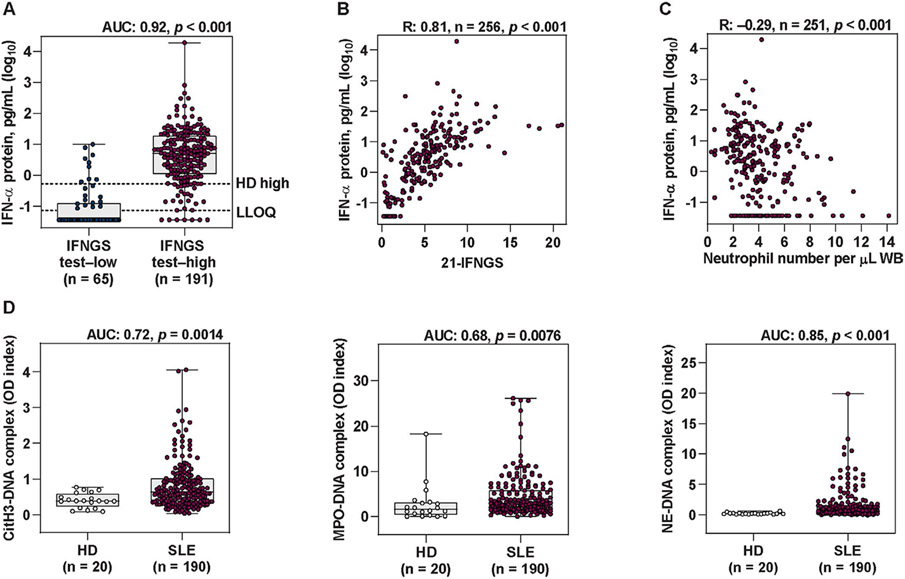
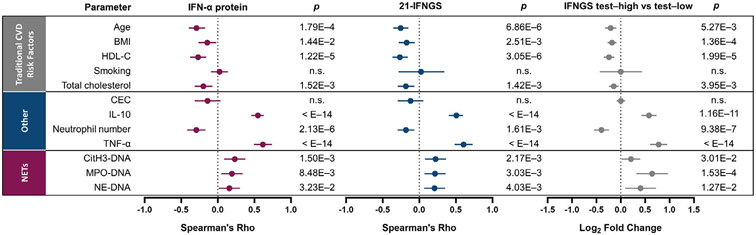
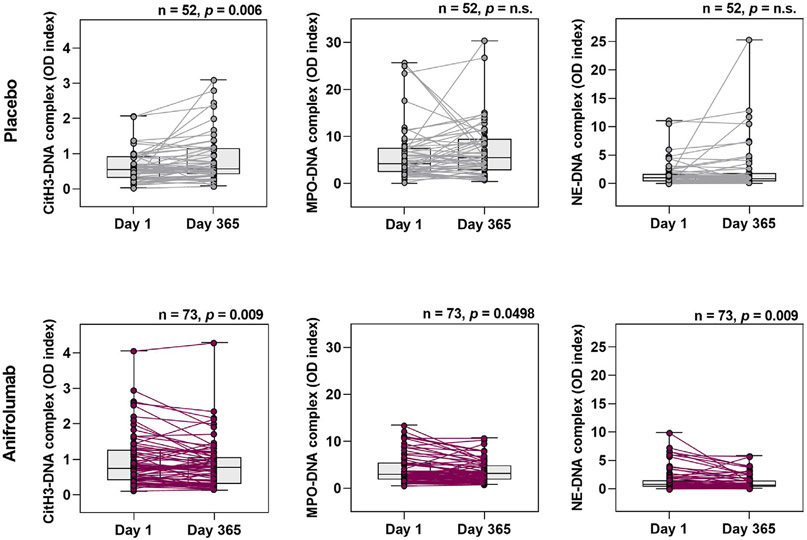
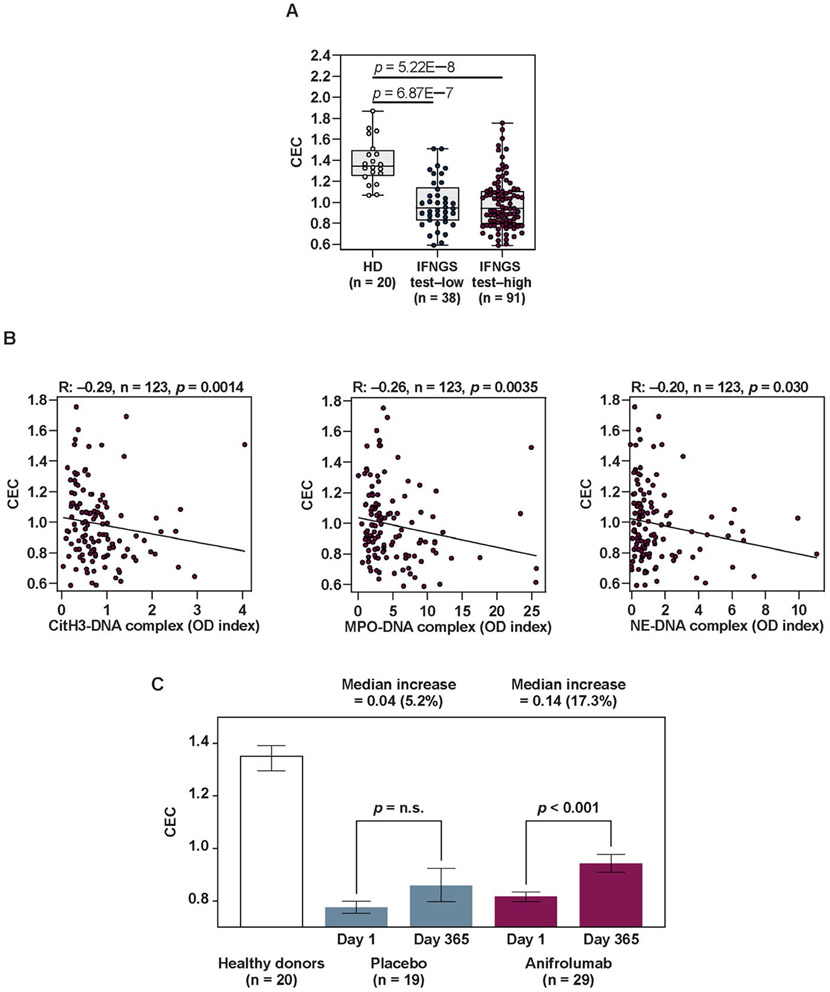
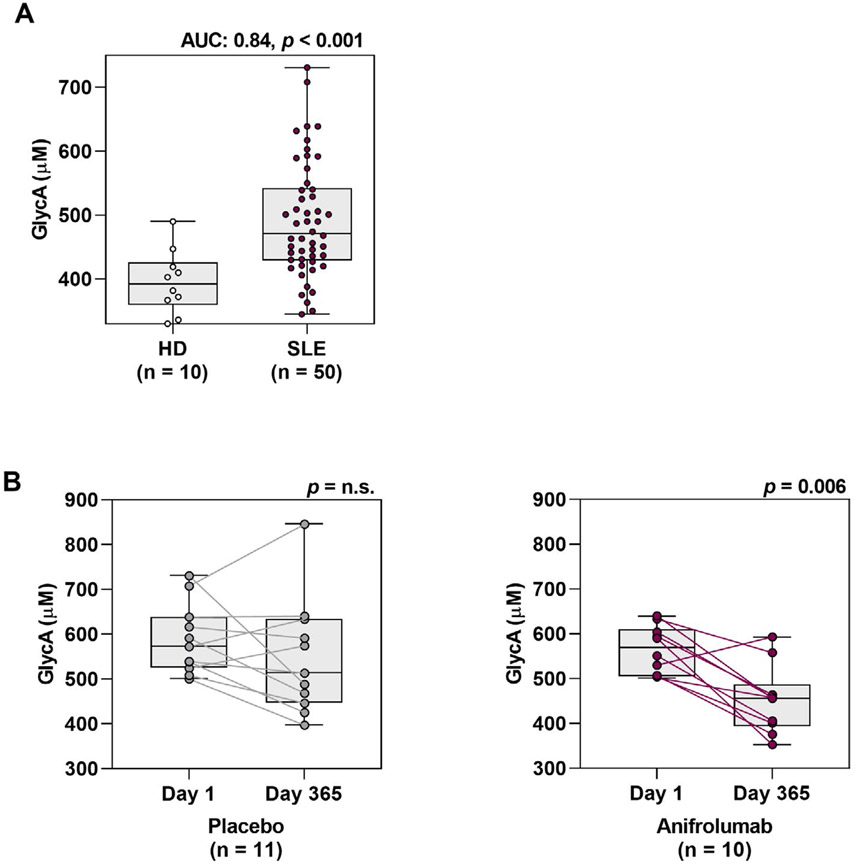
Results: Formation of NET complexes and levels of tumor necrosis factor (TNF) and interleukin-10 (IL-10) were correlated with extent of type I IFN pathway activity. NET complexes and IL-10 levels were up-regulated in SLE patients compared to healthy controls (P < 0.008). The cardiometabolic disease markers CEC and GlycA were also found to be dysregulated in patients with SLE (P < 0.001 versus healthy controls). Type I IFN receptor inhibition with anifrolumab significantly reduced NET complexes and GlycA and improved CEC compared to baseline (P < 0.05) whereas no improvements were seen with placebo. Levels of TNF and IL-10 were reduced with anifrolumab compared to placebo (P < 0.05).
Conclusion: These data support a key role for type I IFNs in modulating factors contributing to SLE vasculopathy and suggest that inhibition of this pathway could decrease cardiovascular risk in individuals with SLE.
Trial registration: ClinicalTrials.gov NCT01438489.
© 2020, American College of Rheumatology.
Figures
References
-
- Nossent J, Cikes N, Kiss E, Marchesoni A, Nassonova V, Mosca M, et al. Current causes of death in systemic lupus erythematosus in Europe, 2000–2004: relation to disease activity and damage accrual. Lupus 2007;16:309–17. - PubMed
-
- Esdaile JM, Abrahamowicz M, Grodzicky T, Li Y, Panaritis C, du Berger R, et al. Traditional Framingham risk factors fail to fully account for accelerated atherosclerosis in systemic lupus erythematosus. Arthritis Rheum 2001;44:2331–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
