

Prospective Comparison of 18F-Choline Positron Emission Tomography/Computed Tomography (PET/CT) and 18F-Fluorodeoxyglucose (FDG) PET/CT in the Initial Workup of Multiple Myeloma: Study Protocol of a Prospective Imaging Trial
- PMID: 32909953
- PMCID: PMC7516691
- DOI: 10.2196/17850
Prospective Comparison of 18F-Choline Positron Emission Tomography/Computed Tomography (PET/CT) and 18F-Fluorodeoxyglucose (FDG) PET/CT in the Initial Workup of Multiple Myeloma: Study Protocol of a Prospective Imaging Trial
Abstract
Background: The International Myeloma Working Group recommends the use of 18-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) for treatment response evaluation, as it is superior to magnetic resonance imaging (MRI). However, at initial staging, the sensitivity of FDG-PET remains inferior to that of MRI. Therefore, there is a need for an imaging technique that could have a sensitivity equal to that of MRI at diagnosis and could serve to evaluate therapy. 18F-choline has shown increased sensitivity when compared with 18-FDG, with about 75% more lesions detected in patients with relapsed or progressive multiple myeloma (MM).
Objective: Our primary objective is to prospectively compare the detection rate of bone lesions by 18F-choline PET/CT (FCH-PET) and FDG-PET in newly diagnosed MM. Our secondary objectives are to assess the accuracy of both PET modalities for the detection of bone lesions and the diagnosis of diffuse disease, to assess the detection rate of extramedullary lesions.
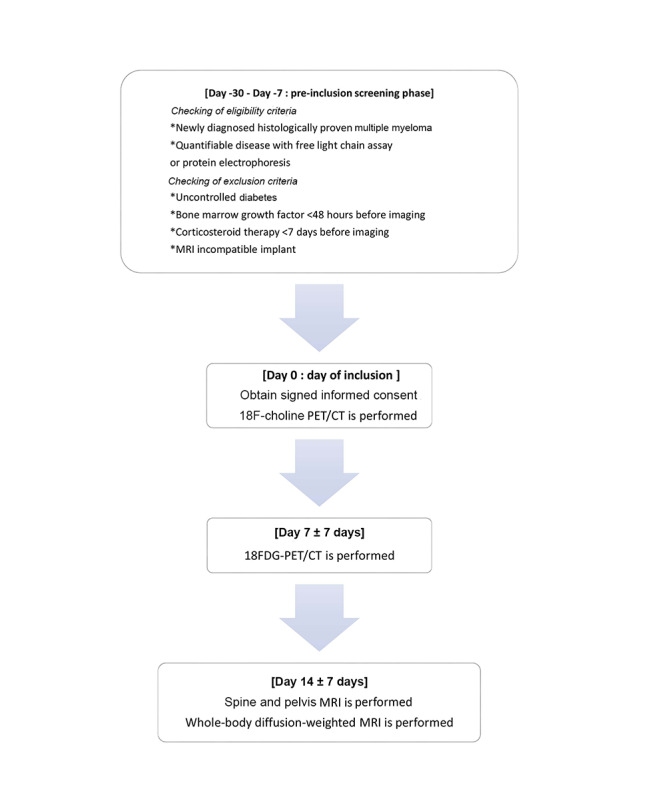
Methods: We will prospectively include 30 patients in a paired comparative accuracy study. Patients with de novo MM will undergo FCH-PET, FDG-PET, and whole-body MRI (WB-MRI) within a 3-week period. WB-MRI will be composed of conventional sequences on the spine and pelvis and of whole-body diffusion axial sequences. The following 6 skeletal areas will be defined: skull, sternum/costal grid, spine, pelvis, superior limbs, and inferior limbs. The number of focal lesions, their respective localization, and intensity of uptake will be retrieved for each skeletal area. Readings will be performed blinded from other imaging techniques. The reference standard will be WB-MRI. Focal lesions present on PET/CT but not on WB-MRI will require a decision made with a consensus of experts based on clinical and imaging data. The number of bone lesions and number of extramedullary lesions will be compared using the Wilcoxon test. The accuracy of FCH-PET and FDG-PET will be compared using the McNemar test.
Results: The study started in September 2019, and enrollment is ongoing. As of June 2020, 8 participants have been included. Data collection is expected to be completed in June 2021, and the results are expected to be available in December 2021.
Conclusions: This study will assess if FCH-PET is superior to FDG-PET for the evaluation of MM tumor burden. This will pave the way for future prospective evaluations of the prognostic value of 18-FCH for treatment response evaluation in MM patients. Additionally, this work may provide new perspectives for better assessment of the risk of smoldering MM progressing to MM.
Trial registration: ClinicalTrials.gov NCT03891914; https://clinicaltrials.gov/ct2/show/NCT03891914.
International registered report identifier (irrid): DERR1-10.2196/17850.
Keywords: 18-FDG; 18F-choline; MRI; PET/CT; cancer; medical imaging; multiple myeloma; skeletal system.
©Charles Mesguich, Cyrille Hulin, Valerie Latrabe, Julien Asselineau, Laurence Bordenave, Paul Perez, Elif Hindie, Gerald Marit. Originally published in JMIR Research Protocols (http://www.researchprotocols.org), 10.09.2020.
Conflict of interest statement
Conflicts of Interest: Curium Pharma graciously provided 20 doses of 18F-choline.
Figures
References
-
- Fonseca R, Abouzaid S, Bonafede M, Cai Q, Parikh K, Cosler L, Richardson P. Trends in overall survival and costs of multiple myeloma, 2000-2014. Leukemia. 2017 Sep;31(9):1915–1921. doi: 10.1038/leu.2016.380. http://europepmc.org/abstract/MED/28008176 - DOI - PMC - PubMed
-
- Kumar SK, Dispenzieri A, Lacy MQ, Gertz MA, Buadi FK, Pandey S, Kapoor P, Dingli D, Hayman SR, Leung N, Lust J, McCurdy A, Russell SJ, Zeldenrust SR, Kyle RA, Rajkumar SV. Continued improvement in survival in multiple myeloma: changes in early mortality and outcomes in older patients. Leukemia. 2014 May;28(5):1122–8. doi: 10.1038/leu.2013.313. http://europepmc.org/abstract/MED/24157580 - DOI - PMC - PubMed
-
- Greipp PR, San Miguel J, Durie BGM, Crowley JJ, Barlogie B, Bladé Joan, Boccadoro M, Child JA, Avet-Loiseau H, Harousseau J, Kyle RA, Lahuerta JJ, Ludwig H, Morgan G, Powles R, Shimizu K, Shustik C, Sonneveld P, Tosi P, Turesson I, Westin J. International staging system for multiple myeloma. J Clin Oncol. 2005 May 20;23(15):3412–20. doi: 10.1200/JCO.2005.04.242. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
