

Optical Coherence Tomography Neuro-Toolbox for the Diagnosis and Management of Papilledema, Optic Disc Edema, and Pseudopapilledema
- PMID: 32909979
- PMCID: PMC7882012
- DOI: 10.1097/WNO.0000000000001078
Optical Coherence Tomography Neuro-Toolbox for the Diagnosis and Management of Papilledema, Optic Disc Edema, and Pseudopapilledema
Abstract
Background: Distinguishing optic disc edema from pseudopapilledema is a common, sometimes challenging clinical problem. Advances in spectral-domain optical coherence tomography (SD-OCT) of the optic nerve head (ONH) has proven to be a cost effective, noninvasive, outpatient procedure that may help. At its core are tools that quantify the thickness of the retinal nerve fiber layer (RNFL) and ganglion cell-inner plexiform layer (GC-IPL). The SD-OCT also provides a set of tools that may be qualitatively interpreted in the same way that we read an MRI. They include the transverse axial, en face, and circular tomogram. Our goal is to describe a practical office-based set of tools using SD-OCT in the diagnosis and monitoring of papilledema, optic disc edema, and pseudopapilledema.
Evidence acquisition: Searches on PubMed were performed using combinations of the following key words: OCT, papilledema, pseudopapilledema, optic disc drusen, retinal folds (RF), and choroidal folds (CF).
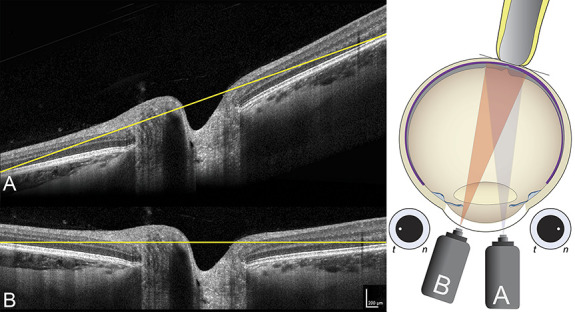
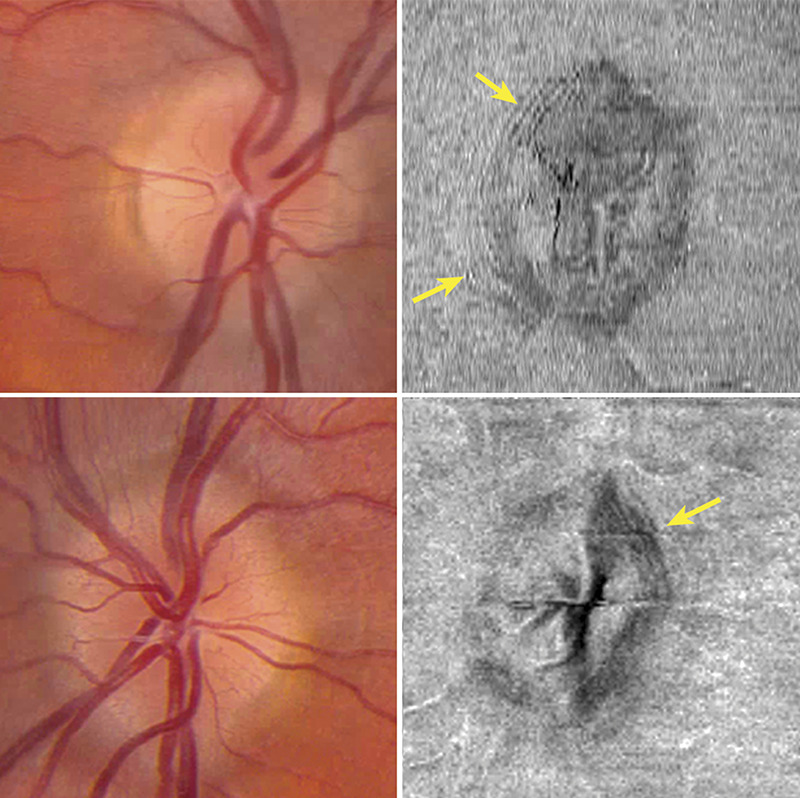
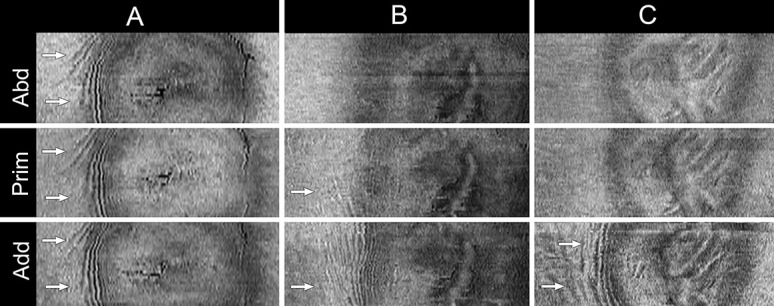
Results: The principal elements of SD-OCT analysis of the ONH are the RNFL and GC-IPL thickness; however, these metrics have limitations when swelling is severe. Qualitative interpretation of the transverse axial SD-OCT aids in assessing peripapillary shape that may help distinguish papilledema from pseudopapilledema, evaluate atypical optic neuropathies, diagnose shunt failures, and identify outer RF and CF. There is a consensus that the SD-OCT is the most sensitive way of identifying buried optic disc drusen. En face SD-OCT is especially effective at detecting peripapillary wrinkles and outer retinal creases, both of which are common and distinctive signs of optic disc edema that rule out pseudopapilledema. Mechanically stressing the ONH in the adducted eye position, in patients with papilledema, may expose folds and peripapillary deformations that may not be evident in primary position. We also discuss how to optimize the acquisition and registration of SD-OCT images.
Conclusions: The SD-OCT is not a substitute for a complete history and a careful examination. It is, however, a convenient ancillary test that aids in the diagnosis and management of papilledema, optic disc edema, and pseudopapilledema. It is particularly helpful in monitoring changes over the course of time and distinguishing low-grade papilledema from buried drusen. The application of the SD-OCT toolbox depends on optimizing the acquisition of images, understanding its limitations, recognizing common artifacts, and accurately interpreting images in the context of both history and clinical findings.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the North American Neuro-Opthalmology Society.
Conflict of interest statement
P. A. Sibony received honorariums from Heidelberg Engineering for invited lectures in 2018. Heidelberg Engineering has provided unrestricted educational and research support to the Department of Neurology at Mt Sinai Medical Center (M. J. Kupersmith and P. A. Sibony) and Department of Ophthalmology University of Iowa (R. H. Kardon). This review does not refer to nor endorse any specific commercial OCT device.
Figures












Comment in
-
Anterior displacement of Bruch's membrane: a useful sign for intracranial hypertension in craniosynostosis.Eye (Lond). 2023 Feb;37(2):369-370. doi: 10.1038/s41433-022-02148-6. Epub 2022 Jul 1. Eye (Lond). 2023. PMID: 35778606 Free PMC article. No abstract available.
References
-
- Kardon R. Optical coherence tomography in papilledema: what am I missing? J Neuroophthalmol. 2014;34(suppl l):S10–S17. - PubMed
-
- Costello F, Malmqvist L, Hamann S. The role of optical coherence tomography in differentiating optic disc drusen from optic disc edema. Asia Pac J Ophthalmol. 2018;7:271–279. - PubMed
-
- Chen JJ. Optical coherence tomography and neuro-ophthalmology. J Neuroophthalmol. 2018;38:e5–e8. - PubMed
-
- Chen JJ, Costello F. The role of optical coherence tomography in neuro-ophthalmology. Ann Eye Sci. 2018;3:1–18.
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
