

Iron deficiency after kidney transplantation
- PMID: 32910168
- PMCID: PMC8577626
- DOI: 10.1093/ndt/gfaa123
Iron deficiency after kidney transplantation
Abstract
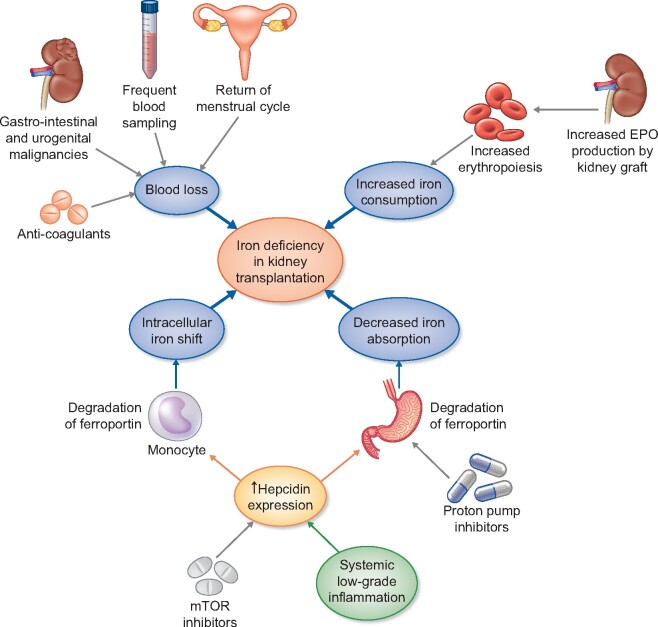
Iron deficiency (ID) is highly prevalent in kidney transplant recipients (KTRs) and has been independently associated with an excess mortality risk in this population. Several causes lead to ID in KTRs, including inflammation, medication and an increased iron need after transplantation. Although many studies in other populations indicate a pivotal role for iron as a regulator of the immune system, little is known about the impact of ID on the immune system in KTRs. Moreover, clinical trials in patients with chronic kidney disease or heart failure have shown that correction of ID, with or without anaemia, improves exercise capacity and quality of life, and may improve survival. ID could therefore be a modifiable risk factor to improve graft and patient outcomes in KTRs; prospective studies are warranted to substantiate this hypothesis.
Keywords: fibroblast growth factor-23; heart failure; immunity; iron; kidney transplantation.
© The Author(s) 2020. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
References
-
- Eisenga MF, Minović I, Berger SP. et al.. Iron deficiency, anemia, and mortality in renal transplant recipients. Transpl Int 2016; 29: 1176–1183 - PubMed
-
- Winkelmayer WC, Lorenz M, Kramar R. et al.. Percentage of hypochromic red blood cells is an independent risk factor for mortality in kidney transplant recipients. Am J Transplant 2004; 4: 2075–2081 - PubMed
-
- Camaschella C. Iron deficiency. Blood 2019; 133: 30–39 - PubMed
-
- Macdougall IC, Bock AH, Carrera F. et al..; on behalf of the FIND-CKD Study Investigators. FIND-CKD: a randomized trial of intravenous ferric carboxymaltose versus oral iron in patients with chronic kidney disease and iron deficiency anaemia. Nephrol Dial Transplant 2014; 29: 2075–2084 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
