

Effect of Recombinant Human Granulocyte Colony-Stimulating Factor for Patients With Coronavirus Disease 2019 (COVID-19) and Lymphopenia: A Randomized Clinical Trial
- PMID: 32910179
- PMCID: PMC7489414
- DOI: 10.1001/jamainternmed.2020.5503
Effect of Recombinant Human Granulocyte Colony-Stimulating Factor for Patients With Coronavirus Disease 2019 (COVID-19) and Lymphopenia: A Randomized Clinical Trial
Abstract
Importance: Lymphopenia is common and correlates with poor clinical outcomes in patients with coronavirus disease 2019 (COVID-19).
Objective: To determine whether a therapy that increases peripheral blood leukocyte and lymphocyte cell counts leads to clinical improvement in patients with COVID-19.
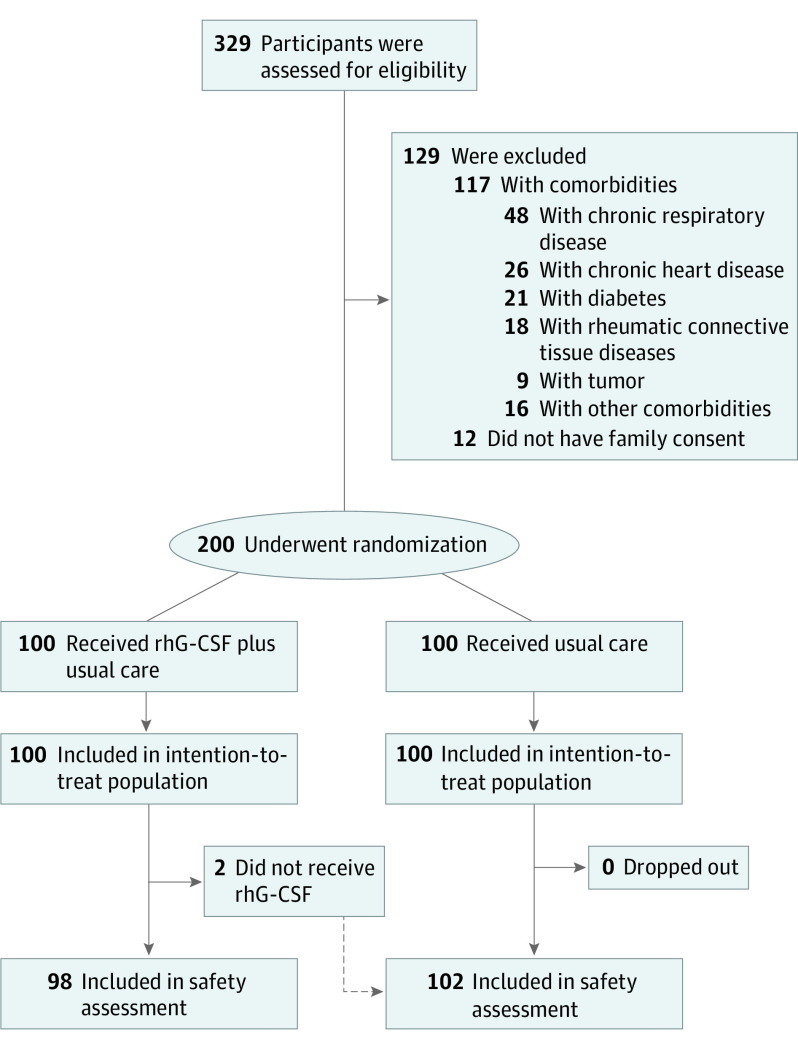
Design, setting and participants: Between February 18 and April 10, 2020, we conducted an open-label, multicenter, randomized clinical trial at 3 participating centers in China. The main eligibility criteria were pneumonia, a blood lymphocyte cell count of 800 per μL (to convert to ×109/L, multiply by 0.001) or lower, and no comorbidities. Severe acute respiratory syndrome coronavirus 2 infection was confirmed with reverse-transcription polymerase chain reaction testing.
Exposures: Usual care alone, or usual care plus 3 doses of recombinant human granulocyte colony-stimulating factor (rhG-CSF, 5 μg/kg, subcutaneously at days 0-2).
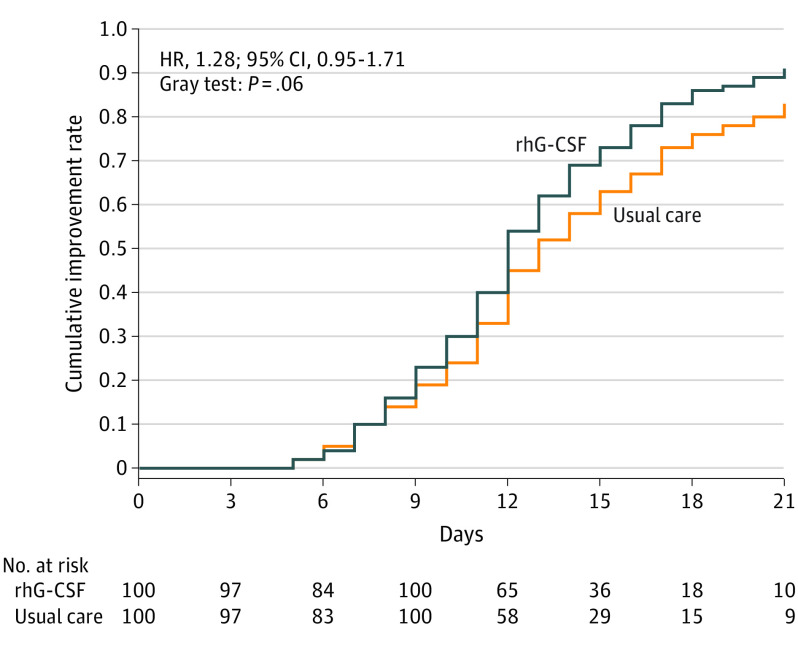
Main outcomes and measures: The primary end point was the time from randomization to improvement of at least 1 point on a 7-category disease severity score.
Results: Of 200 participants, 112 (56%) were men and the median (interquartile range [IQR]) age was 45 (40-55) years. There was random assignment of 100 patients (50%) to the rhG-CSF group and 100 (50%) to the usual care group. Time to clinical improvement was similar between groups (rhG-CSF group median of 12 days (IQR, 10-16 days) vs usual care group median of 13 days (IQR, 11-17 days); hazard ratio, 1.28; 95% CI, 0.95-1.71; P = .06). For secondary end points, the proportion of patients progressing to acute respiratory distress syndrome, sepsis, or septic shock was lower in the rhG-CSF group (rhG-CSF group, 2% vs usual care group, 15%; difference, -13%; 95%CI, -21.4% to -5.4%). At 21 days, 2 patients (2%) had died in the rhG-CSF group compared with 10 patients (10%) in the usual care group (hazard ratio, 0.19; 95%CI, 0.04-0.88). At day 5, the lymphocyte cell count was higher in the rhG-CSF group (rhG-CSF group median of 1050/μL vs usual care group median of 620/μL; Hodges-Lehmann estimate of the difference in medians, 440; 95% CI, 380-490). Serious adverse events, such as sepsis or septic shock, respiratory failure, and acute respiratory distress syndrome, occurred in 29 patients (14.5%) in the rhG-CSF group and 42 patients (21%) in the usual care group.
Conclusion and relevance: In preliminary findings from a randomized clinical trial, rhG-CSF treatment for patients with COVID-19 with lymphopenia but no comorbidities did not accelerate clinical improvement, but the number of patients developing critical illness or dying may have been reduced. Larger studies that include a broader range of patients with COVID-19 should be conducted.
Trial registration: Chinese Clinical Trial Registry: ChiCTR2000030007.
Conflict of interest statement
Figures
Comment in
-
Immune Stimulation With Recombinant Human Granulocyte Colony-Stimulating Factor for Coronavirus Disease 2019 (COVID-19)-Beware of Blind Spots.JAMA Intern Med. 2021 Jan 1;181(1):78-80. doi: 10.1001/jamainternmed.2020.5536. JAMA Intern Med. 2021. PMID: 32910155 No abstract available.
References
-
- World Health Organization WHO coronavirus disease (COVID-19) dashboard. Accessed August 11, 2020. https://covid19.who.int/
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
