

Severe acute pancreatitis: surgical indications and treatment
- PMID: 32910276
- PMCID: PMC8106572
- DOI: 10.1007/s00423-020-01944-6
Severe acute pancreatitis: surgical indications and treatment
Abstract
Background: Acute pancreatitis (AP) is defined as an acute inflammatory attack of the pancreas of sudden onset. Around 25% of patients have either moderately severe or severe disease with a mortality rate of 15-20%.
Purpose: The aim of this article was to summarize the advances being made in the understanding of this disease and the important role of surgery.
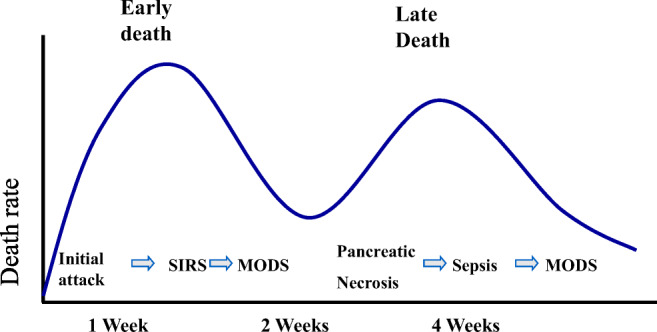
Results and conclusions: An accurate diagnosis should be made a soon as possible, initiating resuscitation with large volume intravenous fluids and oxygen by mask. Predicted severe disease will require intensive monitoring. Most deaths within the first week are due to multi-organ failure; thus, these patients will require intensive therapy unit management. During the second phase of the disease, death is due to local complications arising from the pancreatic inflammation, requiring accurate identification to determine the correct form of treatment. Acute peripancreatic fluid collections arise < 4 weeks after onset of interstitial edematous pancreatitis, not requiring any treatment. Most pancreatic pseudocysts arise > 4 weeks and largely resolve on conservative management. Necrotizing pancreatitis causing acute necrotic collections and later walled-off necrosis will require treatment if symptomatic or infected. Initial endoscopic transgastric or percutaneous drainage will resolve less serious collections but necrosectomy using minimally invasive approaches will be needed for more serious collections. To prevent recurrent attacks of AP, causative factors need to be removed where possible such as cholecystectomy and cessation of alcohol. Future progress requires improved management of multi-organ failure and more effective minimally invasive techniques for the removal of necrosis.
Keywords: Endoscopic; Infection; Minimally invasive surgery; Necrosectomy; Pancreatic necrosis; Percutaneous.
Conflict of interest statement
Dr. Heckler has nothing to disclose; Prof. Dr. med. Hackert has nothing to disclose; Dr. Hu has nothing to disclose; Dr. Halloran reports grants from Cancer Research UK, grants from Pancreatic Cancer UK, grants from the NIHR-RfPb, and grants from the Royal College of Surgeons of England, all outside the submitted work; Prof. Dr. med. Büchler reports Board Membership of B. Braun Melsungen GmbH, outside the submitted work; Prof. Dr. med. Neoptolemos reports grants from the Heidelberger Stiftung Chirurgie, grants from NUCANA, and grants from the Stiftung Deutsche Krebshilfe, all outside the submitted work; .
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
