

Physiology-Based Treatment of Myoclonus
- PMID: 32910414
- PMCID: PMC7851206
- DOI: 10.1007/s13311-020-00922-6
Physiology-Based Treatment of Myoclonus
Abstract
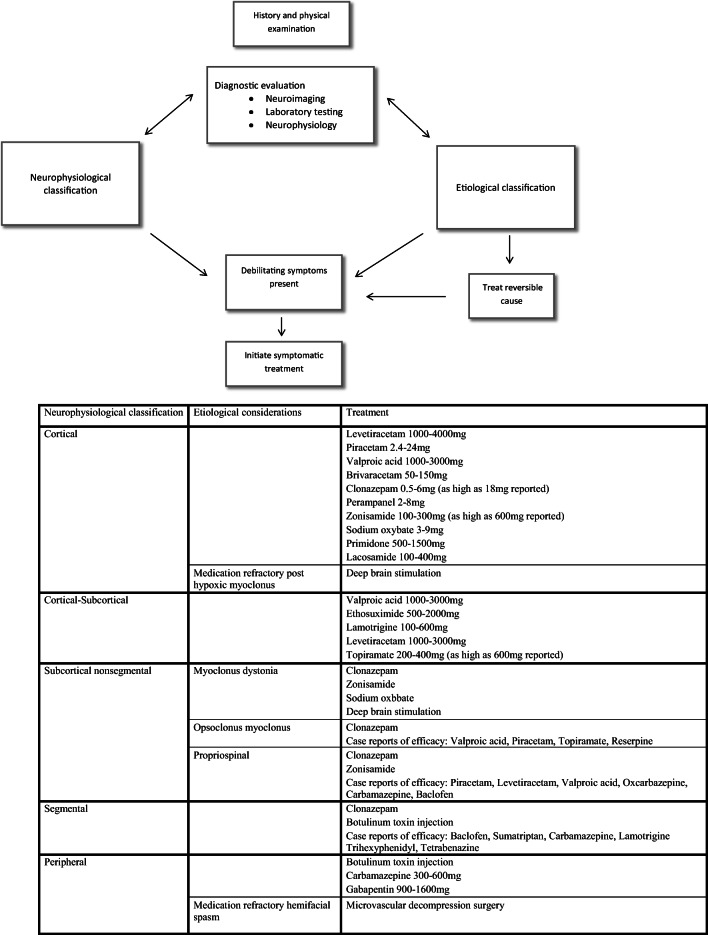
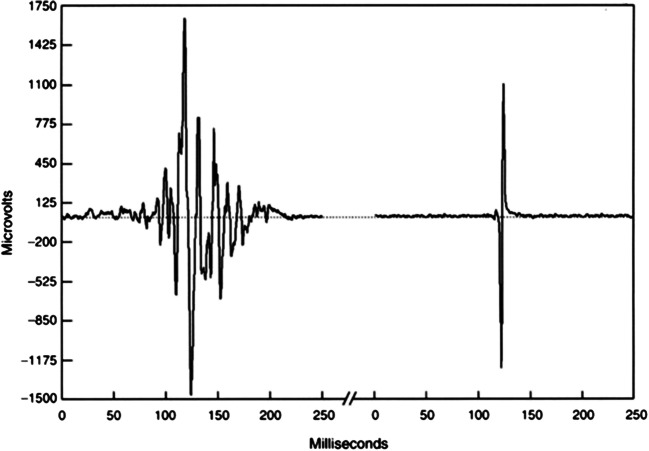
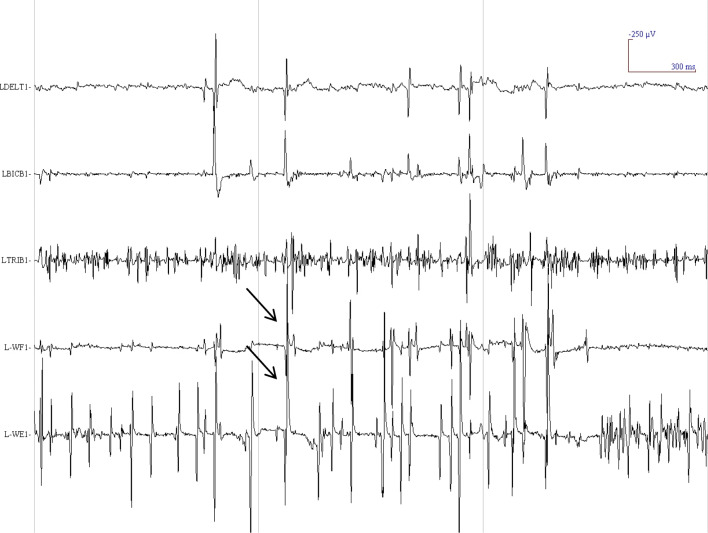
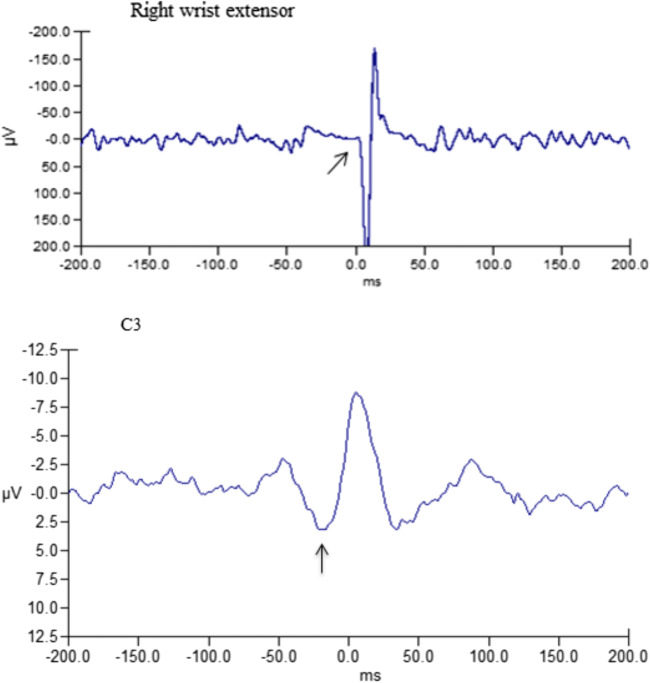
Myoclonus can cause significant disability for patients. Myoclonus has a strikingly diverse array of underlying etiologies, clinical presentations, and pathophysiological mechanisms. Treatment of myoclonus is vital to improving the quality of life of patients with these disorders. The optimal treatment strategy for myoclonus is best determined based upon careful evaluation and consideration of the underlying etiology and neurophysiological classification. Electrophysiological testing including EEG (electroencephalogram) and EMG (electromyogram) data is helpful in determining the neurophysiological classification of myoclonus. The neurophysiological subtypes of myoclonus include cortical, cortical-subcortical, subcortical-nonsegmental, segmental, and peripheral. Levetiracetam, valproic acid, and clonazepam are often used to treat cortical myoclonus. In cortical-subcortical myoclonus, treatment of myoclonic seizures is prioritized, valproic acid being the mainstay of therapy. Subcortical-nonsegmental myoclonus may be treated with clonazepam, though numerous agents have been used depending on the etiology. Segmental and peripheral myoclonus are often resistant to treatment, but anticonvulsants and botulinum toxin injections may be of utility depending upon the case. Pharmacological treatments are often hampered by scarce evidence-based knowledge, adverse effects, and variable efficacy of medications.
Keywords: EEG; EMG; Myoclonus; neurophysiology; treatment.
Figures
Similar articles
-
Treatment of myoclonus.Neurotherapeutics. 2014 Jan;11(1):188-200. doi: 10.1007/s13311-013-0216-3. Neurotherapeutics. 2014. PMID: 24037428 Free PMC article. Review.
-
Rhythmic EMG and EEG activity during voluntary movement in posthypoxic cortical action myoclonus.J UOEH. 2005 Sep 1;27(3):227-36. doi: 10.7888/juoeh.27.227. J UOEH. 2005. PMID: 16180509
-
Myoclonus.Handb Clin Neurol. 2011;100:399-420. doi: 10.1016/B978-0-444-52014-2.00031-8. Handb Clin Neurol. 2011. PMID: 21496598 Review.
-
Clinical presentations and phenomenology of myoclonus.Epilepsia. 2003;44 Suppl 11:7-12. doi: 10.1046/j.1528-1157.44.s11.3.x. Epilepsia. 2003. PMID: 14641566 Review.
-
Electrophysiological studies of myoclonus.Muscle Nerve. 2005 Feb;31(2):157-74. doi: 10.1002/mus.20234. Muscle Nerve. 2005. PMID: 15547927 Review.
Cited by
-
Myoclonus Secondary to Amantadine: Case Report and Literature Review.Clin Pract. 2023 Jul 20;13(4):830-837. doi: 10.3390/clinpract13040075. Clin Pract. 2023. PMID: 37489424 Free PMC article.
-
Myoclonus: Differential diagnosis and current management.Epilepsia Open. 2024 Apr;9(2):486-500. doi: 10.1002/epi4.12917. Epub 2024 Feb 9. Epilepsia Open. 2024. PMID: 38334331 Free PMC article. Review.
-
Myoclonus and other jerky movement disorders.Clin Neurophysiol Pract. 2022 Oct 6;7:285-316. doi: 10.1016/j.cnp.2022.09.003. eCollection 2022. Clin Neurophysiol Pract. 2022. PMID: 36324989 Free PMC article. Review.
-
Antiseizure Drugs and Movement Disorders.CNS Drugs. 2022 Aug;36(8):859-876. doi: 10.1007/s40263-022-00937-x. Epub 2022 Jul 21. CNS Drugs. 2022. PMID: 35861924 Review.
-
Post hypoxic myoclonus: A tale of two minds.Epilepsy Behav Rep. 2023 Jan 21;21:100589. doi: 10.1016/j.ebr.2023.100589. eCollection 2023. Epilepsy Behav Rep. 2023. PMID: 36747905 Free PMC article.
References
-
- Marsden CD, Hallett M, Fahn S. The nosology and pathophysiology of myoclonus. In: Marsden CD, Fahn S, editors. Movement Disorders. London: Butterworths; 1983. pp. 196–248.
-
- Caviness JN, Brown P. Myoclonus: current concepts and recent advances. Lancet Neurol. 2004;3:598–607. - PubMed
-
- Caviness JN Clinical neurophysiology of myoclonus. In: Hallett M, editor. Movement Disorders. Handbook of Clinical Neurophysiology. Amsterdam: Elsevier; 2003. pp. 521–548.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
