

Continuous Versus 1-Year Fixed-Duration Nivolumab in Previously Treated Advanced Non-Small-Cell Lung Cancer: CheckMate 153
- PMID: 32910710
- PMCID: PMC7676888
- DOI: 10.1200/JCO.20.00131
Continuous Versus 1-Year Fixed-Duration Nivolumab in Previously Treated Advanced Non-Small-Cell Lung Cancer: CheckMate 153
Abstract
Purpose: Limited data exist on the optimal duration of immunotherapy, including for non-small-cell lung cancer (NSCLC). We present an exploratory analysis of CheckMate 153, a largely community-based phase IIIb/IV study, to evaluate the impact of 1-year fixed-duration versus continuous therapy on the efficacy and safety of nivolumab.
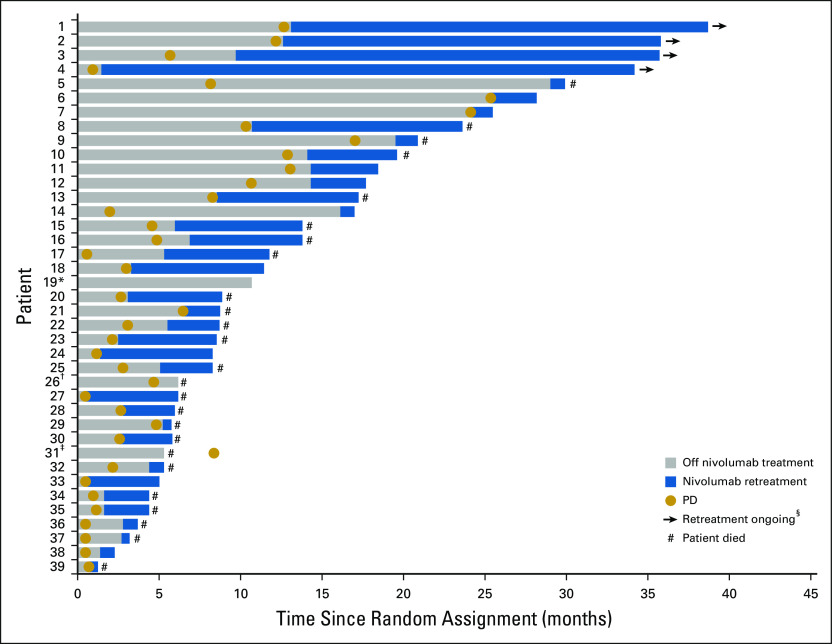
Methods: Patients with previously treated advanced NSCLC received nivolumab monotherapy (3 mg/kg every 2 weeks). Those still receiving treatment at 1 year, including patients perceived to be deriving benefit despite radiographic progression, were randomly assigned to continue nivolumab until disease progression or unacceptable toxicity or to stop nivolumab with the option of on-study retreatment after disease progression (1-year fixed duration).
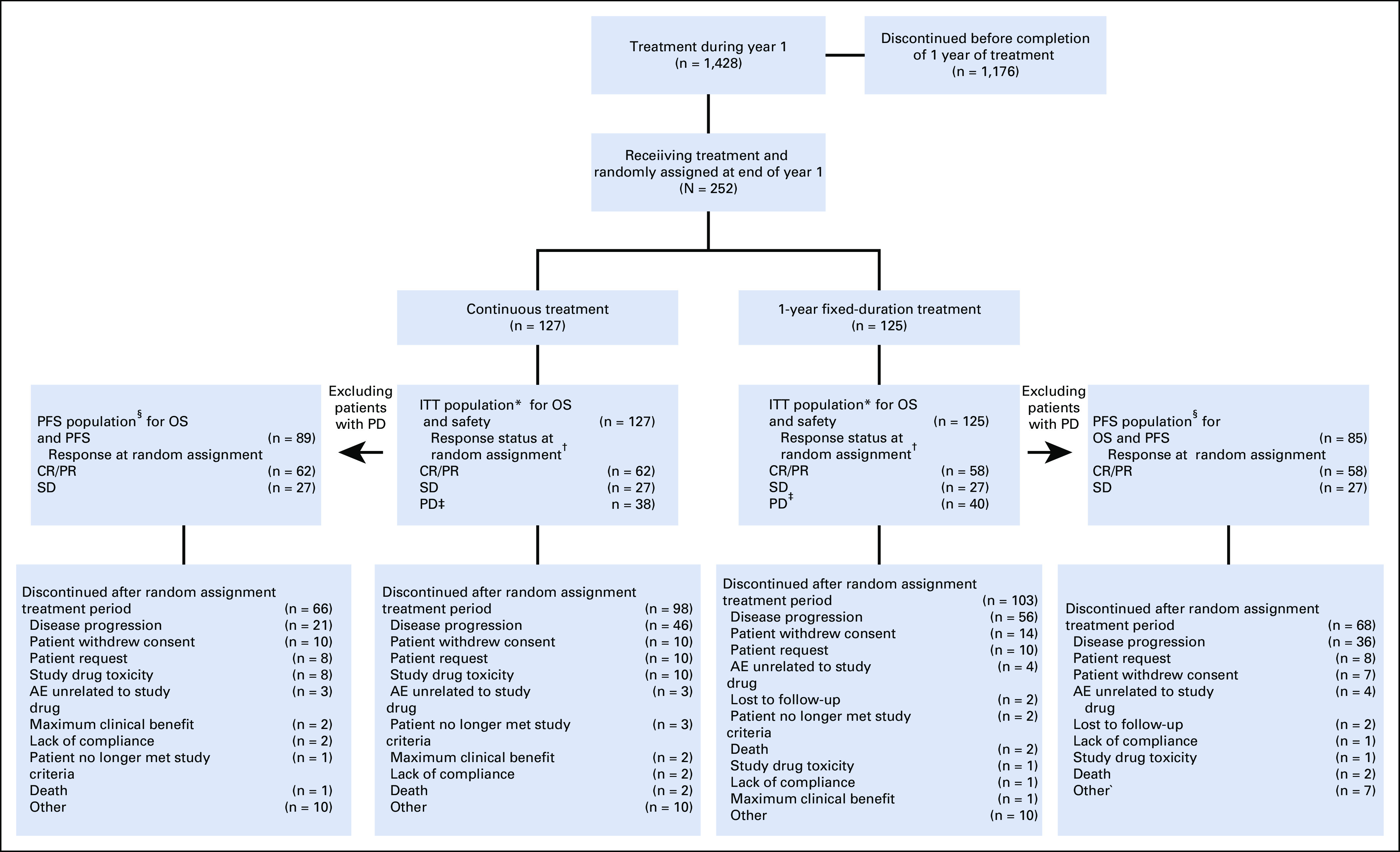
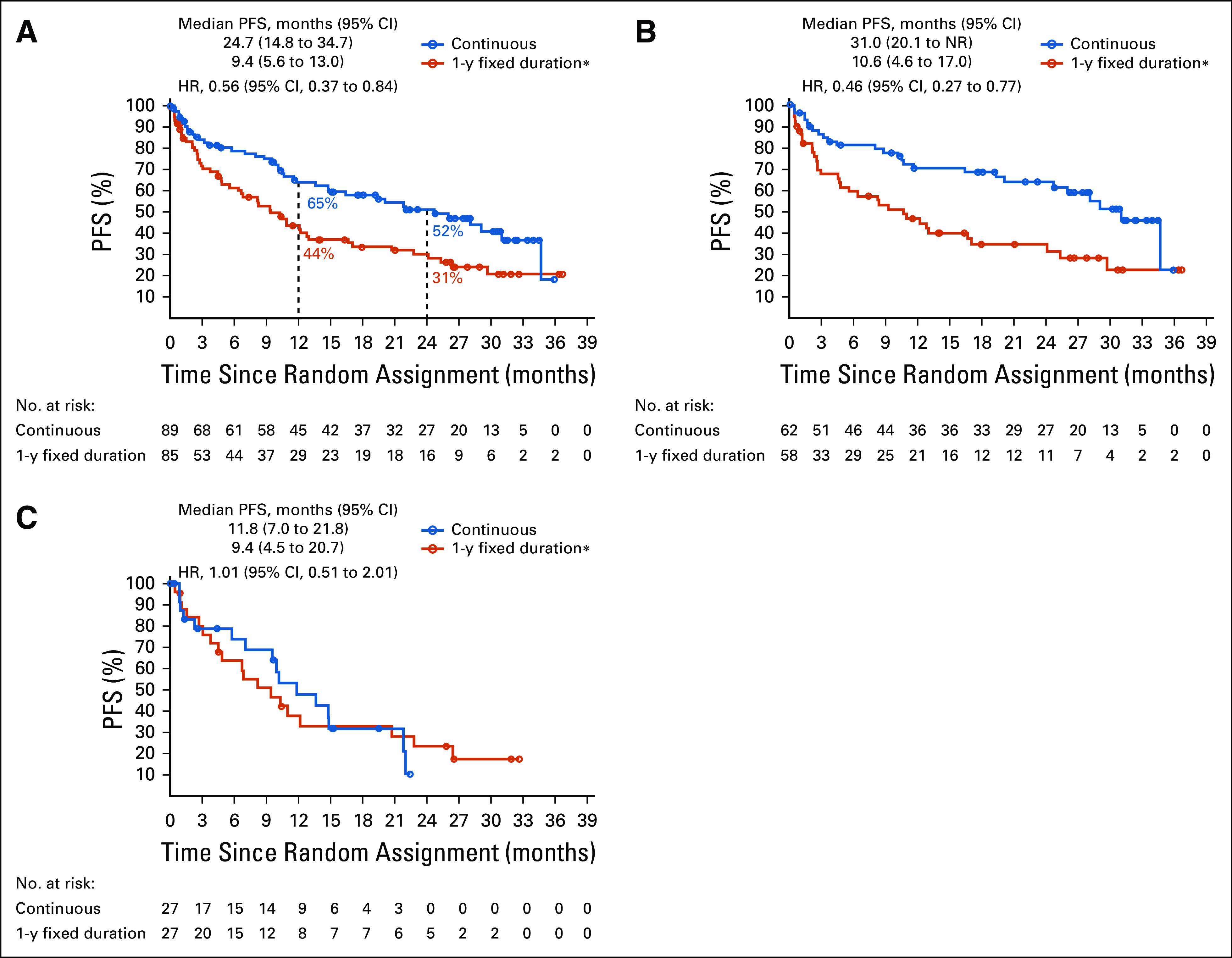
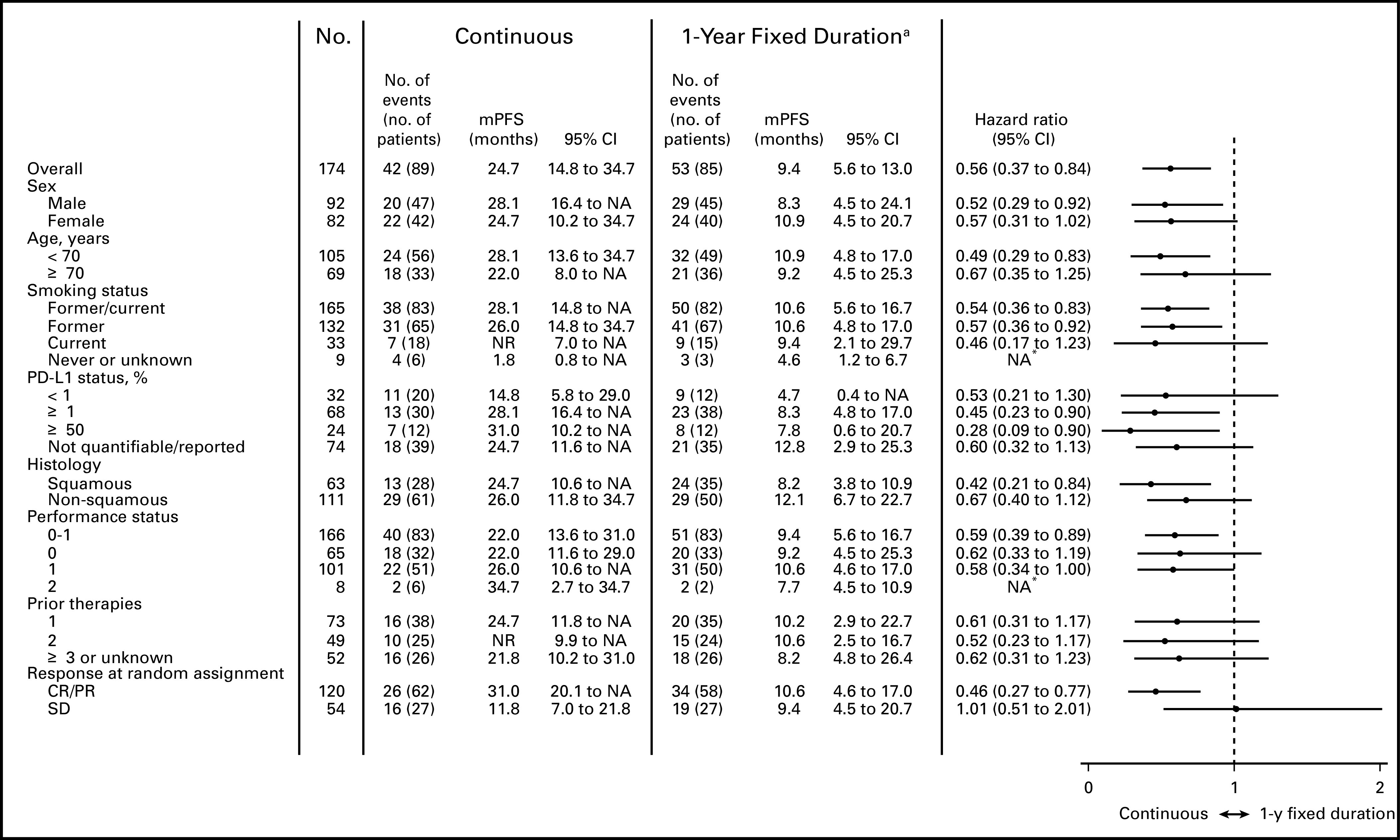
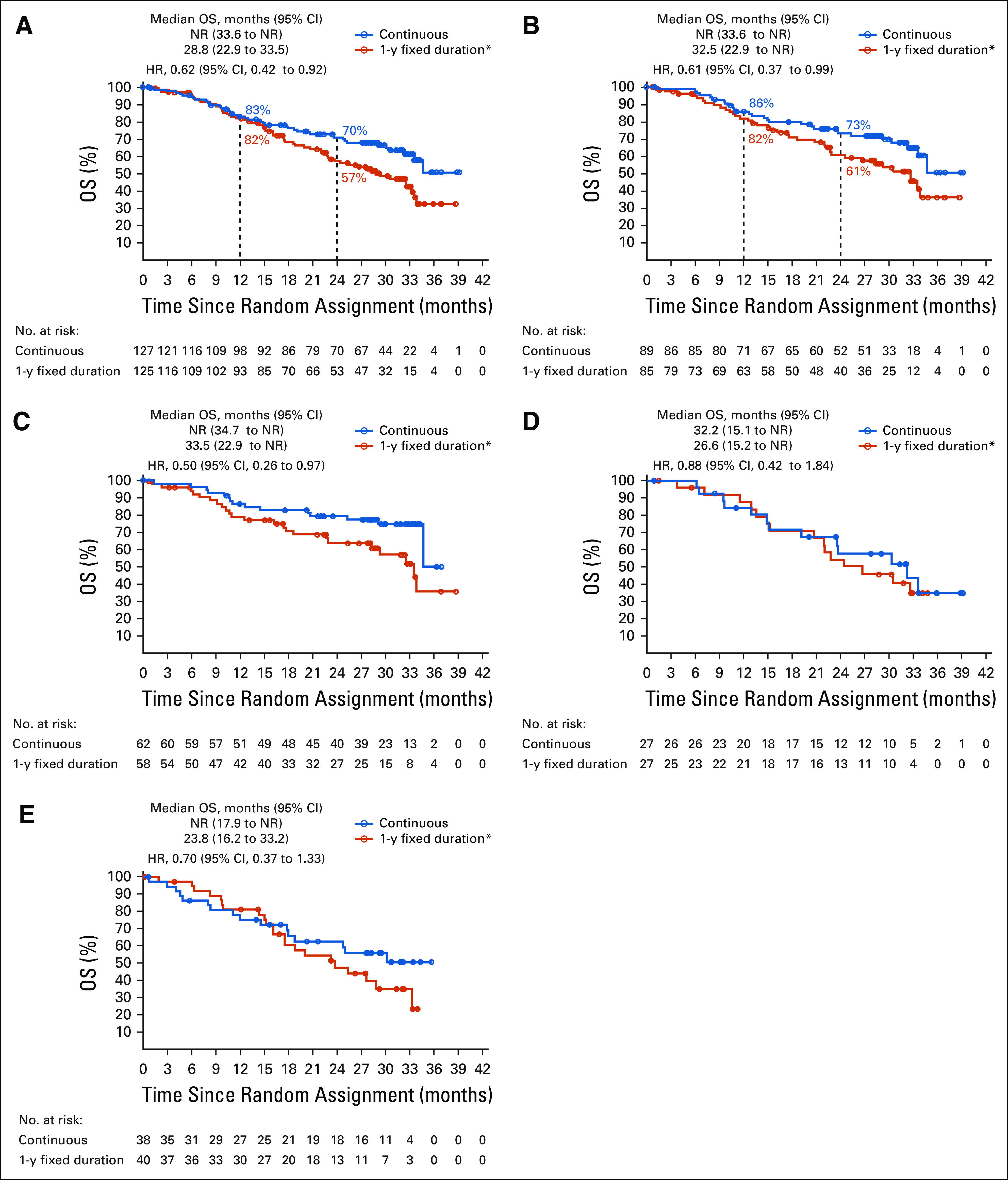
Results: Of 1,428 patients treated, 252 were randomly assigned to continuous (n = 127) or 1-year fixed-duration (n = 125) treatment (intent-to-treat [ITT] population). Of these, 89 and 85 patients in the continuous and 1-year fixed-duration arms, respectively, had not progressed (progression-free survival [PFS] population). With minimum post-random assignment follow-up of 13.5 months, median PFS was longer with continuous versus 1-year fixed-duration treatment (PFS population: 24.7 months v 9.4 months; hazard ratio [HR], 0.56 [95% CI, 0.37 to 0.84]). Median overall survival from random assignment was longer with continuous versus 1-year fixed-duration treatment in the PFS (not reached v 32.5 months; HR, 0.61 [95% CI, 0.37 to 0.99]) and ITT (not reached v 28.8 months; HR, 0.62 [95% CI, 0.42 to 0.92]) populations. Few new-onset treatment-related adverse events occurred. No new safety signals were identified.
Conclusion: To our knowledge, these findings from an exploratory analysis represent the first randomized data on continuous versus fixed-duration immunotherapy in previously treated advanced NSCLC and suggest that continuing nivolumab beyond 1 year improves outcomes.
Conflict of interest statement
Continuous Versus 1-Year Fixed-Duration Nivolumab in Previously Treated Advanced Non–Small-Cell Lung Cancer: CheckMate 153
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
David M. Waterhouse
Edward B. Garon
Jason Chandler
Maen Hussein
Robert Jotte
Leora Horn
Davey B. Daniel
George Keogh
Ben Creelan
Lawrence H. Einhorn
Samer Kasbari
Felix Couture
Natasha B. Leighl
Craig Reynolds
George Blumenschein Jr
Nivedita Aanur
David R. Spigel
No other potential conflicts of interest were reported.
Figures
Comment in
-
To Continue or Not to Continue? That Is the Question.J Clin Oncol. 2020 Nov 20;38(33):3830-3832. doi: 10.1200/JCO.20.02191. Epub 2020 Sep 30. J Clin Oncol. 2020. PMID: 32997574 No abstract available.
References
-
- Bristol Myers Squibb Company: Opdivo (nivolumab) prescribing information, June 2020. https://packageinserts.bms.com/pi/pi_opdivo.pdf.
-
- National Comprehensive Cancer Network : Non-small Cell Lung Cancer, Volume 1. National Comprehensive Cancer Network 2019. https://www.nccn.org/professionals/physician_gls/default.aspx
-
- Borghaei H Brahmer JR Chow LQM, et al. : Five-year outcomes from the randomized, phase 3 trials CheckMate 017/057: Nivolumab vs docetaxel in previously treated NSCLC. Presented at the IASLC 20th World Conference on Lung Cancer, Barcelona, Spain, September 10, 2019
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
