

Different independent associations of depression and anxiety with survival in patients with cancer
- PMID: 32911441
- PMCID: PMC7614809
- DOI: 10.1016/j.jpsychores.2020.110218
Different independent associations of depression and anxiety with survival in patients with cancer
Abstract
Objective: Depression and anxiety have both been reported to predict worse subsequent survival in people with cancer. However, depression and anxiety are mutually associated and we lack understanding of their independent associations with survival. We therefore aimed to investigate these in a large sample of patients with common cancers.
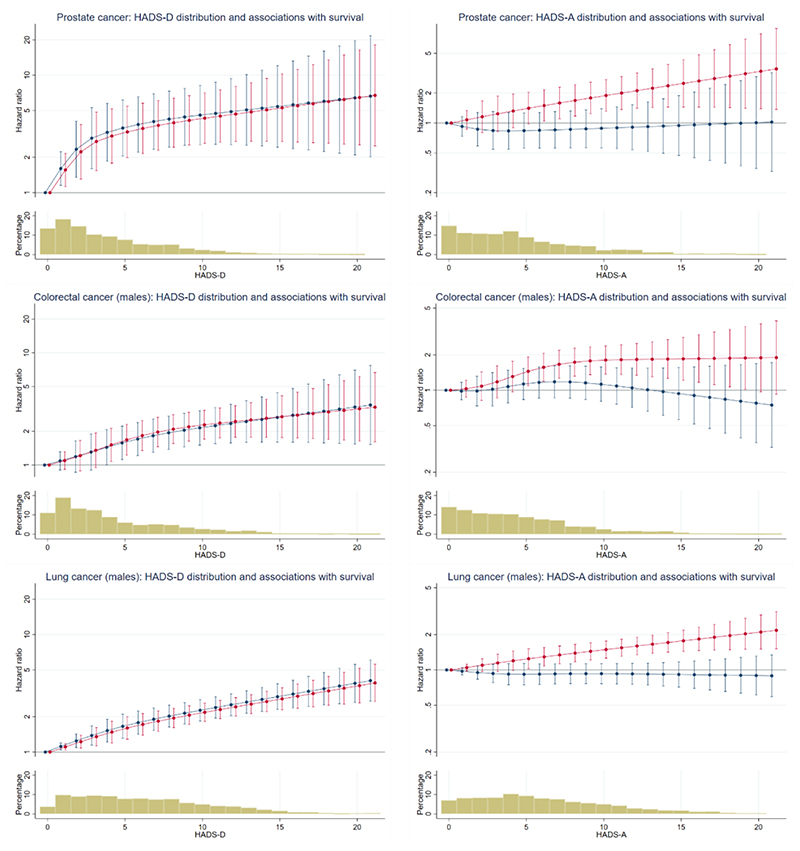
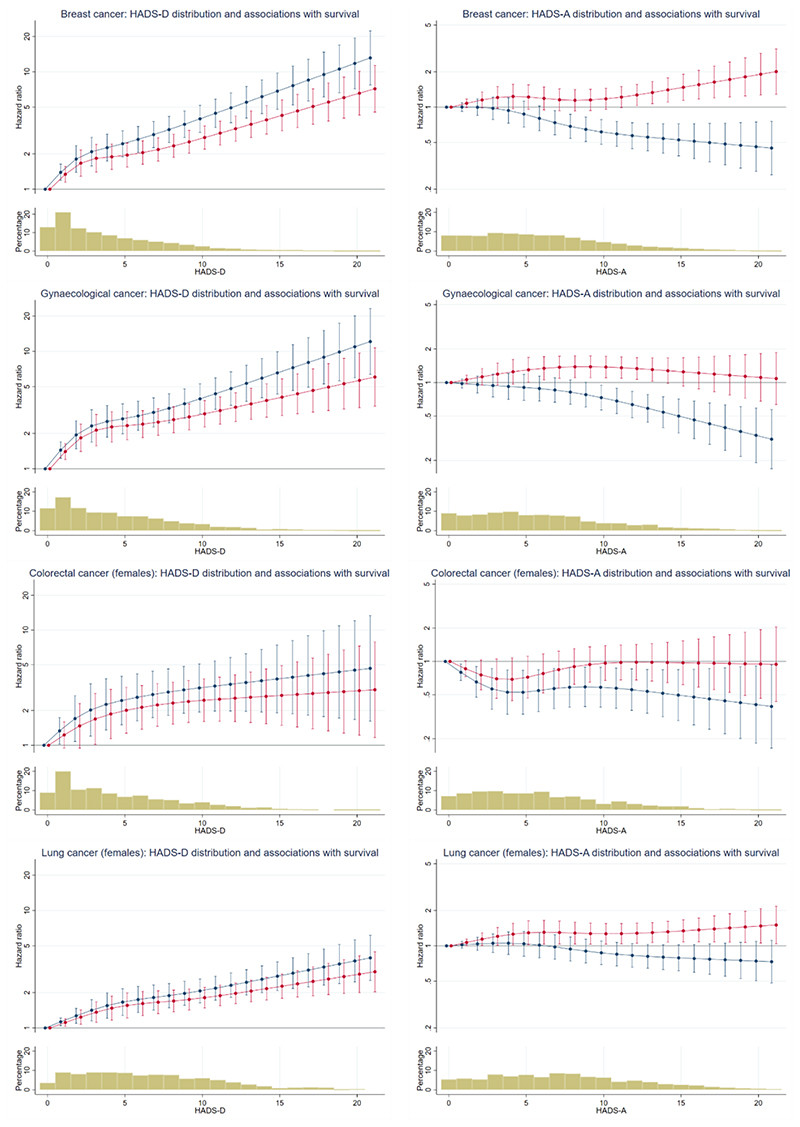
Methods: We analysed data on 19,966 patients with common cancers (breast, colorectal, gynaecological, lung and prostate) who had attended specialist NHS outpatient clinics in Scotland, UK. Hospital Anxiety and Depression Scale (HADS) data were linked with demographic, cancer and mortality data. We estimated the independent associations of depression (HADS depression score) and anxiety (HADS anxiety score) with survival by fitting (separately for each cancer) Cox proportional hazards models which incorporated cubic splines to allow for non-linear associations. We also adjusted for potential confounders.
Results: The median time from HADS completion to death or censoring was 1.9 years. Greater depression was found to be strongly associated with worse survival from all cancers. When adjusted for anxiety, this association remained in males and increased in females. Greater anxiety was also associated with worse survival in nearly all cancers. However, when adjusted for depression, the association of anxiety with worse survival was lost. In females the association reversed direction so that greater anxiety was associated with better survival.
Conclusion: Although often considered together as aspects of 'emotional distress', depression and anxiety have different independent associations with survival in patients with cancer and should therefore be considered separately.
Keywords: Anxiety; Cancer; Depression; Mortality; Neoplasms; Survival.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest None.
Figures
References
-
- Satin JR, Linden W, Phillips MJ. Depression as a predictor of disease progression and mortality in cancer patients: a meta-analysis. Cancer. 2009;115(22):5349–61. - PubMed
-
- Wang YH, Li JQ, Shi JF, Que JY, Liu JJ, Lappin JM, Leung J, Ravindran AV, Chen WQ, Qiao YL, Shi J, et al. Depression and anxiety in relation to cancer incidence and mortality: a systematic review and meta-analysis of cohort studies. Mol Psychiatry. 2019 - PubMed
-
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica. 1983;67:361–370. - PubMed
