Three Rare Concurrent Complications of Tertiary Hyperparathyroidism: Maxillary Brown Tumor, Uremic Leontiasis Ossea, and Hungry Bone Syndrome
- PMID: 32911586
- PMCID: PMC7571245
- DOI: 10.11005/jbm.2020.27.3.217
Three Rare Concurrent Complications of Tertiary Hyperparathyroidism: Maxillary Brown Tumor, Uremic Leontiasis Ossea, and Hungry Bone Syndrome
Abstract
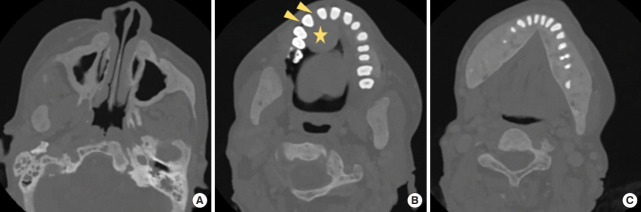
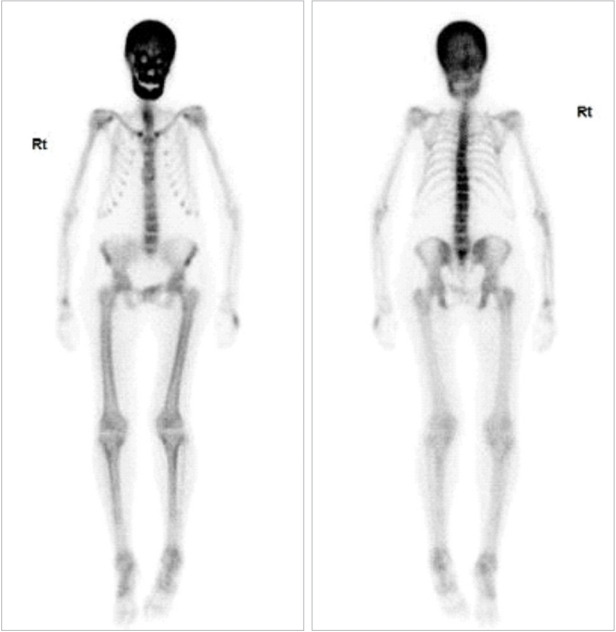
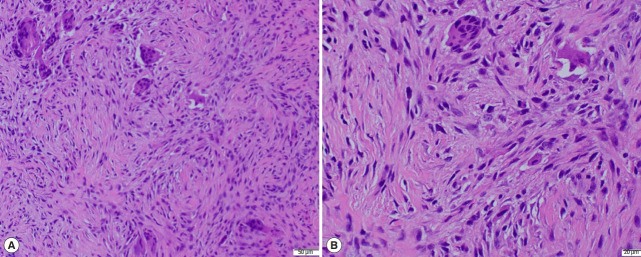
A 48-year-old woman in her 40's with end-stage renal disease and tertiary hyperparathyroidism (HPT) presented for a rapidly progressive maxillary tumor. Initial workup was notable for elevated intact parathyroid hormone (PTH) and diffuse thickening of skull and facial bones on computed tomography, and maxillary tumor biopsy with multinucleated giant cells. She underwent subtotal parathyroidectomy (with removal of a parathyroid adenoma and 2 hyperplastic glands) and partial resection of maxillary brown tumor. The patient's post-operative course was complicated by hungry bone syndrome, with hypocalcemia refractory to aggressive calcium repletion. Teriparatide (recombinant PTH) was utilized with rapid resolution of hypocalcemia. To our knowledge, this is the first case of maxillary brown tumor in tertiary HPT to be reported in the USA. This case also supports teriparatide as a novel therapeutic for hungry bone syndrome refractory to aggressive calcium repletion.
Keywords: Brown tumor; Hungry bone syndrome; Maxilla; Teriparatide; Tertiary hyperparathyroidism; Uremic leontiasis ossea.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures

Similar articles
-
Uremic leontiasis ossea due to secondary hyperparathyroidism complicated by vitamin C deficiency in a non-adherent chronic hemodialysis patient: A case report.Clin Nephrol Case Stud. 2019 Sep 9;7:54-59. doi: 10.5414/CNCS109788. eCollection 2019. Clin Nephrol Case Stud. 2019. PMID: 31508269 Free PMC article.
-
Use of Recombinant Human Parathyroid Hormone to Treat Hungry Bone Syndrome in Hemodialysis Patient.Oman Med J. 2020 Jul 31;35(4):e164. doi: 10.5001/omj.2020.106. eCollection 2020 Jul. Oman Med J. 2020. PMID: 32904907 Free PMC article.
-
Uremic Leontiasis Ossea due to Resistant Secondary Hyperparathyroidism.AACE Clin Case Rep. 2024 Sep 12;11(1):5-9. doi: 10.1016/j.aace.2024.09.001. eCollection 2025 Jan-Feb. AACE Clin Case Rep. 2024. PMID: 39896948 Free PMC article.
-
Brown tumors of the jaws associated with primary or secondary hyperparathyroidism. A clinical study and review of the literature.Am J Otolaryngol. 2006 Jul-Aug;27(4):281-6. doi: 10.1016/j.amjoto.2005.11.004. Am J Otolaryngol. 2006. PMID: 16798410 Review.
-
Hungry bone syndrome.Curr Opin Nephrol Hypertens. 2017 Jul;26(4):250-255. doi: 10.1097/MNH.0000000000000327. Curr Opin Nephrol Hypertens. 2017. PMID: 28375869 Review.
Cited by
-
Multiple fractures due to hungry bone syndrome following parathyroidectomy: a clinical case report and review of literature.Clin Diabetes Endocrinol. 2024 Aug 17;10(1):25. doi: 10.1186/s40842-024-00183-8. Clin Diabetes Endocrinol. 2024. PMID: 39152506 Free PMC article.
-
Forestalling Hungry Bone Syndrome after Parathyroidectomy in Patients with Primary and Renal Hyperparathyroidism.Diagnostics (Basel). 2023 Jun 2;13(11):1953. doi: 10.3390/diagnostics13111953. Diagnostics (Basel). 2023. PMID: 37296804 Free PMC article. Review.
-
A Rare Presentation of a Bi-Maxillary Brown Tumour due to Secondary Hyperparathyroidism.Case Rep Dent. 2023 Mar 27;2023:6180006. doi: 10.1155/2023/6180006. eCollection 2023. Case Rep Dent. 2023. PMID: 37021075 Free PMC article.
-
The value of integration of bone scan and targeted SPECT/CT in diagnosis of primary hyperparathyroidism with multiple bone brown tumor.Skeletal Radiol. 2023 Dec;52(12):2505-2511. doi: 10.1007/s00256-023-04361-0. Epub 2023 May 25. Skeletal Radiol. 2023. PMID: 37227482
-
Brown Tumors: The Hidden Face of Primary and Renal Hyperparathyroidism Amid Real-Life Settings.J Clin Med. 2024 Jun 29;13(13):3847. doi: 10.3390/jcm13133847. J Clin Med. 2024. PMID: 38999413 Free PMC article.
References
-
- Abdel Razek AA. Computed tomography and magnetic resonance imaging of maxillofacial lesions in renal osteodystrophy. J Craniofac Surg. 2014;25:1354–7. - PubMed
-
- Han YH, Jeong HJ, Lim ST, et al. Uremic leontiasis ossea in a patient with chronic renal insufficiency demonstrated on bone scintigraphy. Clin Nucl Med. 2016;41:641–2. - PubMed
-
- Lee VS, Webb MS, Jr., Martinez S, et al. Uremic leontiasis ossea: “bighead” disease in humans? Radiologic, clinical, and pathologic features. Radiology. 1996;199:233–40. - PubMed