

Risk prediction for coronary heart disease by a genetic risk score - results from the Heinz Nixdorf Recall study
- PMID: 32912153
- PMCID: PMC7487988
- DOI: 10.1186/s12881-020-01113-y
Risk prediction for coronary heart disease by a genetic risk score - results from the Heinz Nixdorf Recall study
Abstract
Background: A Genetic risk score for coronary artery disease (CAD) improves the ability of predicting coronary heart disease (CHD). It is unclear whether i) the use of a CAD genetic risk score is superior to the measurement of coronary artery calcification (CAC) for CHD risk assessment and ii) the CHD risk assessment using a CAD genetic risk score differs between men and women.
Methods: We included 4041 participants (age-range: 45-76 years, 1919 men) of the Heinz Nixdorf Recall study without CHD or stroke at baseline. A standardized weighted CAD genetic risk score was constructed using 70 known genetic variants. The risk score was divided into quintiles (Q1-Q5). We specified low (Q1), intermediate (Q2-Q4) and high (Q5) genetic risk groups. Incident CHD was defined as fatal and non-fatal myocardial infarction, stroke and coronary death. The association between the genetic risk score and genetic risk groups with incident CHD was assessed using Cox models to estimate hazard ratios (HR) and 95%-confidence intervals (CI). The models were adjusted by age and sex (Model1), as well as by established CHD risk factors (RF) and CAC (Model2). The analyses were further stratified by sex and controlled for multiple testing.
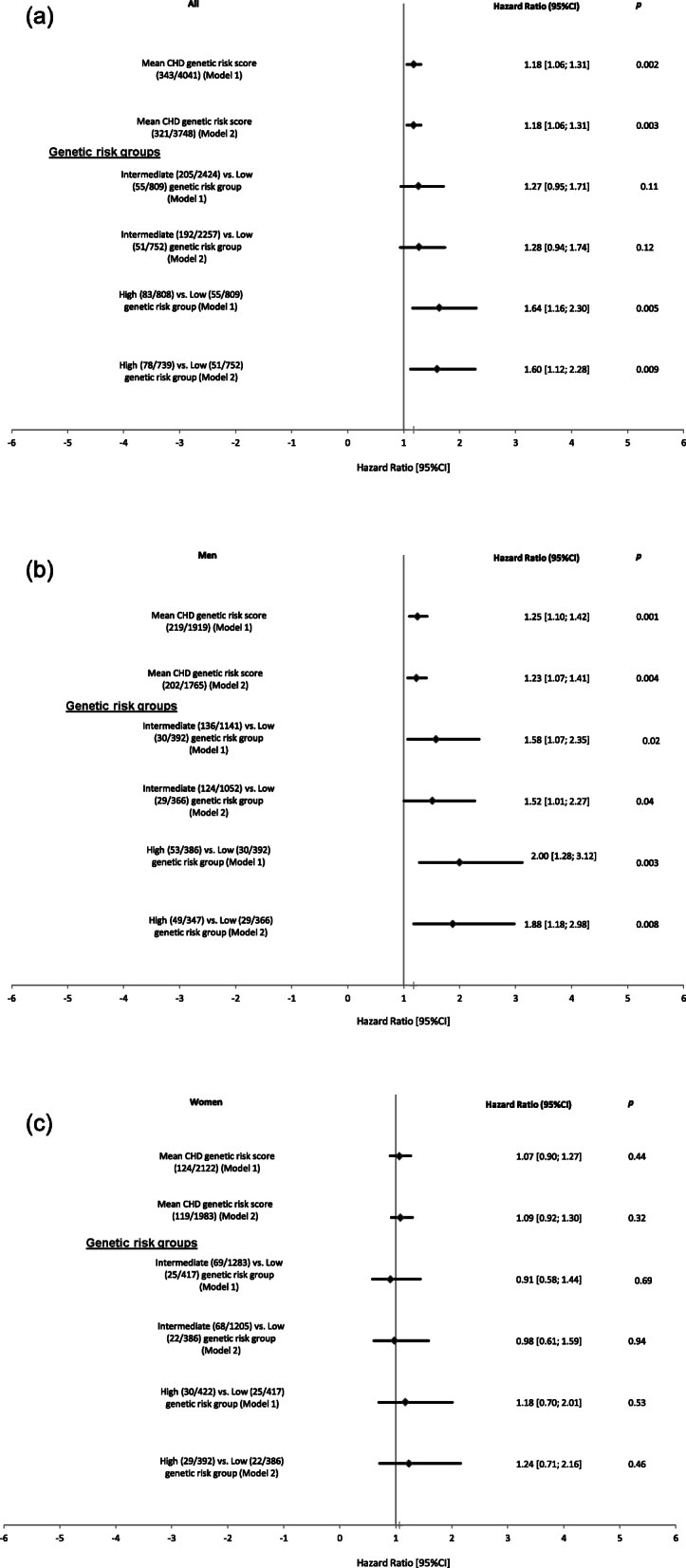
Results: During a median follow-up time of 11.6 ± 3.7 years, 343 participants experienced CHD events (219 men). Per-standard deviation (SD) increase in the genetic risk score was associated with 18% increased risk for incident CHD (Model1: p = 0.002) which did not change after full adjustment (Model2: HR = 1.18 per-SD (p = 0.003)). In Model2 we observed a 60% increased CHD risk in the high (p = 0.009) compared to the low genetic risk group. Stratifying by sex, only men showed statistically significantly higher risk for CHD (Model2: HR = 1.23 per-SD (p = 0.004); intermediate: HR = 1.52 (p = 0.04) and high: HR = 1.88 (p = 0.008)) with no statistically significant risk observed in women.
Conclusion: Our results suggest that the CAD genetic risk score could be useful for CHD risk prediction, at least in men belonging to the higher genetic risk group, but it does not outbalance the value of CT-based quantification of CAC which works independently on both men and women and allows better risk stratification in both the genders.
Keywords: Cohort study; Coronary artery calcification; Coronary artery disease; Coronary heart disease; Genetic risk score.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Wilkins E, Wilson L, Wickramasinghe K, Bhatnagar P, Leal J, Luengo-Fernandez R, Burns R, Rayner M, Townsend N. European Cardiovascular Disease Statistics 2017. European Heart Network Brussels. 2017. http://www.ehnheart.org/cvd-statistics/cvd-statistics-2017.html.
-
- Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR) Atherosclerosis. 2016;252:207–274. doi: 10.1016/j.atherosclerosis.2016.05.037. - DOI - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the Management of Blood Cholesterol: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2018. 10.1016/j.jacc.2018.11.002.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
