

Radiotherapy in oncological emergencies: fast-track treatment planning
- PMID: 32912293
- PMCID: PMC7488151
- DOI: 10.1186/s13014-020-01657-6
Radiotherapy in oncological emergencies: fast-track treatment planning
Abstract
Background and purpose: To report on our clinical experience with a newly implemented workflow for radiotherapy (RT) emergency treatments, which allows for a fast treatment application outside the regular working-hours, and its clinical applicability.
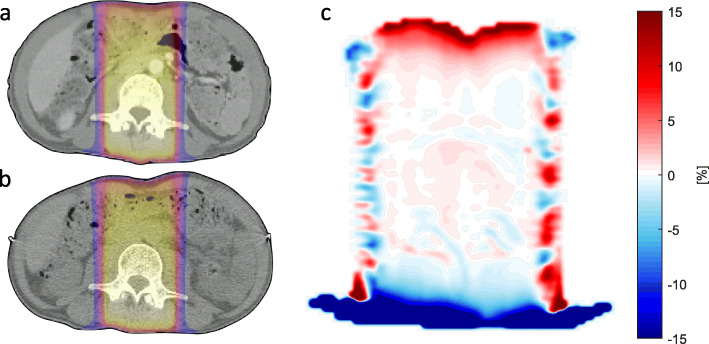
Methods: Treatment planning of 18 emergency RT patients was carried out using diagnostic computed tomography (CT) without a dedicated RT simulation CT. The cone-beam CT (CBCT) deviations of the first RT treatment were analyzed regarding setup accuracy. Furthermore, feasibility of the "fast-track" workflow was evaluated with respect to dose deviations caused by different Hounsfield unit (HU) to relative electron density (rED) calibrations and RT treatment couch surface shapes via 3D gamma index analysis of exemplary treatment plans. The dosimetric uncertainty introduced by different CT calibrations was quantified.
Results: Mean patient setup vs. CBCT isocenter deviations were (0.49 ± 0.44) cm (x), (2.68 ± 1.63) cm (y) and (1.80 ± 1.06) cm (z) for lateral, longitudinal and vertical directions, respectively. Three out of four dose comparisons between the emergency RT plan calculated on the diagnostic CT and the same plan calculated on the treatment planning CT showed clinically acceptable gamma passing rates, when correcting for surface artifacts. The maximum difference of rED was 0.054, while most parts of the CT calibration curves coincided well.
Conclusion: In an emergency RT setting, the use of diagnostic CT data for treatment planning might be time-saving and was shown to be suitable for many cases, considering reproducibility of patient setup, accuracy of initial patient setup and accuracy of dose-calculation.
Keywords: Emergency RT workflow; Emergency radiation treatment; Fast treatment planning; Rapid planning; Treatment planning on diagnostic CT.
Conflict of interest statement
CB and SC received speaker honoraria and research grants from ELEKTA AB (Stockholm, Sweden) and C-Rad AB (Upsala, Sweden). The other authors declare that they have no competing interests.
Figures



References
-
- Christian E, Adamietz IA, Willich N, Schäfer U, Micke O, G. W. G. P. R. of the German Society for Radiation Oncology (DEGRO) Radiotherapy in oncological emergencies-final results of a patterns of care study in Germany, Austria and Switzerland. Acta Oncologica. 2008;47(1):81–89. doi: 10.1080/02841860701481554. - DOI - PubMed
-
- Donato V, Bonfili P, Bulzonetti N, Santarelli M, Osti MF, Tombolini V, Banelli E, Enrici RM. Radiation therapy for oncological emergencies. Anticancer Res. 2001;21(3C):2219–2224. - PubMed
-
- Gao W, Nyflot MJ, Novak A, Sponseller PA, Jordan L, Carlson J, Kane G, Zeng J, Ford EC. Can emergent treatments result in more severe errors?: an analysis of a large institutional near-miss incident reporting database. Pract Radiat Oncol. 2015;5(5):319–324. doi: 10.1016/j.prro.2015.06.008. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
