

Diffuse Leptomeningeal Glioneuronal Tumor of Childhood
- PMID: 32912870
- PMCID: PMC7658820
- DOI: 10.3174/ajnr.A6737
Diffuse Leptomeningeal Glioneuronal Tumor of Childhood
Abstract
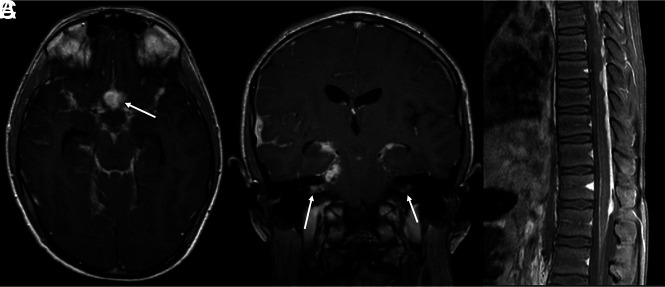
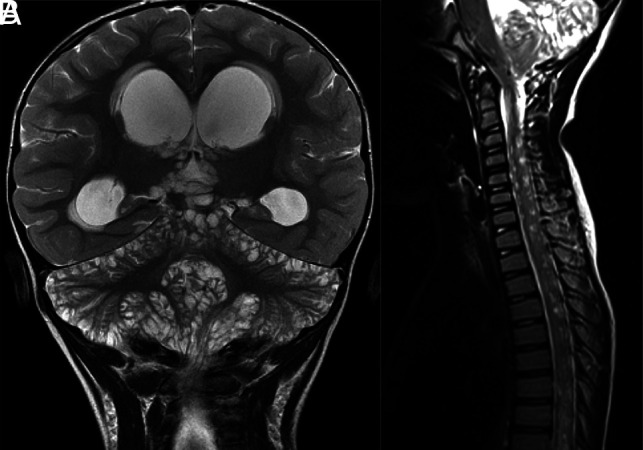
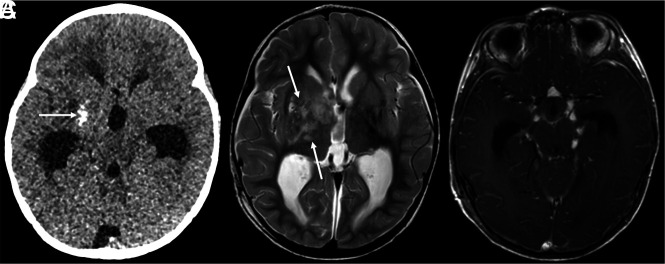
Diffuse leptomeningeal glioneuronal tumor is a newly defined entity under the neuronal and mixed neuronal-glial tumors category in the 2016 World Health Organization classification of brain tumors. In this series, we report clinical, radiologic, and histologic findings in 7 cases of diffuse leptomeningeal glioneuronal tumor. Our cases and literature review indicate that the most characteristic imaging finding is diffuse intracranial and intraspinal nodular leptomeningeal thickening and enhancement. This is often associated with small cyst-like, nonenhancing lesions. It should be noted that tumors sometimes bear nontypical features, for example, presenting as a solitary spinal cord mass without leptomeningeal involvement or with a dominant intracranial mass. In children with characteristic imaging findings and without clinical features of infection, the radiologist has an opportunity to promptly raise the possibility of diffuse leptomeningeal glioneuronal tumor, and thereby, affect streamlined diagnostic evaluation.
© 2020 by American Journal of Neuroradiology.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical