

Changing consumption of resources for respiratory support and short-term outcomes in four consecutive geographical cohorts of infants born extremely preterm over 25 years since the early 1990s
- PMID: 32912950
- PMCID: PMC7488838
- DOI: 10.1136/bmjopen-2020-037507
Changing consumption of resources for respiratory support and short-term outcomes in four consecutive geographical cohorts of infants born extremely preterm over 25 years since the early 1990s
Abstract
Objectives: It is unclear how newer methods of respiratory support for infants born extremely preterm (EP; 22-27 weeks gestation) have affected in-hospital sequelae. We aimed to determine changes in respiratory support, survival and morbidity in EP infants since the early 1990s.
Design: Prospective longitudinal cohort study.
Setting: The State of Victoria, Australia.
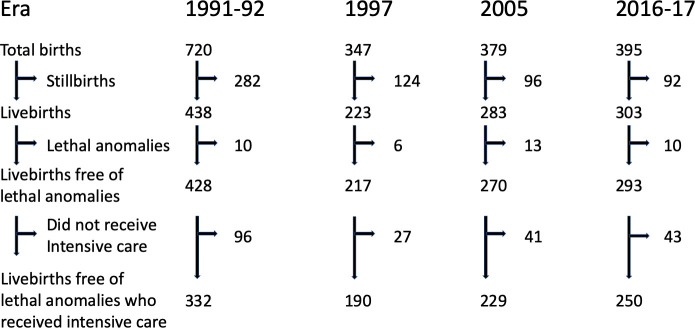
Participants: All EP births offered intensive care in four discrete eras (1991-1992 (24 months): n=332, 1997 (12 months): n=190, 2005 (12 months): n=229, and April 2016-March 2017 (12 months): n=250).
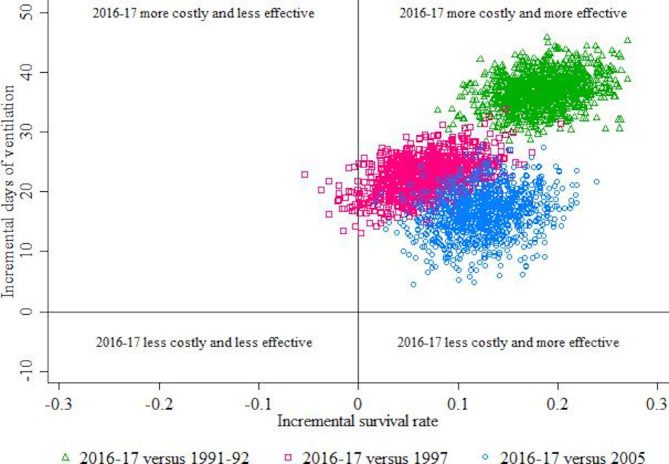
Outcome measures: Consumption of respiratory support, survival and morbidity to discharge home. Cost-effectiveness ratios describing the average additional days of respiratory support associated per additional survivor were calculated.
Results: Median duration of any respiratory support increased from 22 days (1991-1992) to 66 days (2016-2017). The increase occurred in non-invasive respiratory support (2 days (1991-1992) to 51 days (2016-2017)), with high-flow nasal cannulae, unavailable in earlier cohorts, comprising almost one-half of the duration in 2016-2017. Survival to discharge home increased (68% (1991-1992) to 87% (2016-2017)). Cystic periventricular leukomalacia decreased (6.3% (1991-1992) to 1.2% (2016-2017)), whereas retinopathy of prematurity requiring treatment increased (4.0% (1991-1992) to 10.0% (2016-2017)). The average additional costs associated with one additional infant surviving in 2016-2017 were 200 (95% CI 150 to 297) days, 326 (183 to 1127) days and 130 (70 to 267) days compared with 1991-1992, 1997 and 2005, respectively.
Conclusions: Consumption of resources for respiratory support has escalated with improved survival over time. Cystic periventricular leukomalacia reduced in incidence but retinopathy of prematurity requiring treatment increased. How these changes translate into long-term respiratory or neurological function remains to be determined.
Keywords: epidemiology; neonatal intensive & critical care; neonatology.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous