

Microscopic pulmonary tumor embolism from adenocarcinoma of the prostate
- PMID: 32914059
- PMCID: PMC7469864
- DOI: 10.1002/iju5.12159
Microscopic pulmonary tumor embolism from adenocarcinoma of the prostate
Abstract
Introduction: Microscopic pulmonary tumor embolisms from prostate cancer are extremely rare. In this case of prostate cancer, microscopic pulmonary tumor embolism developed during androgen deprivation therapy.
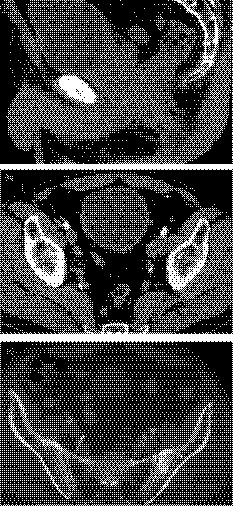
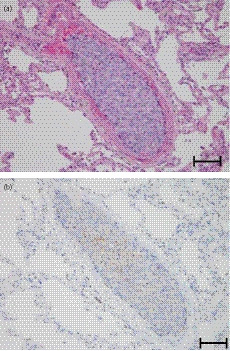
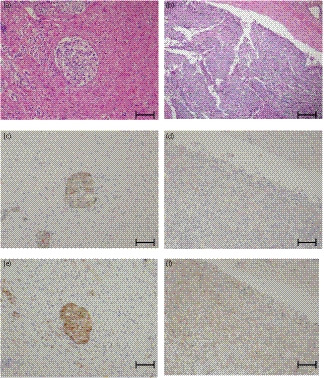
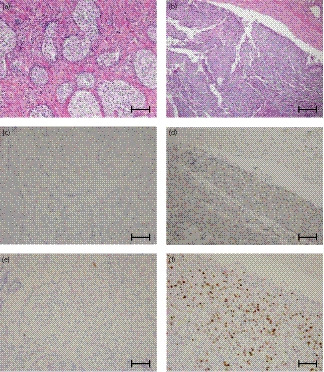
Case presentation: A 56-year-old man was diagnosed with prostate cancer and underwent androgen deprivation therapy. Three months after starting treatment, he noticed shortness of breath and developed acute progressive dyspnea. He was diagnosed with pulmonary hypertension; however, the cause was not found. His dyspnea was progressive and he died 40 days after the onset of symptoms. Autopsy proved that the cause of pulmonary hypertension was microscopic pulmonary tumor emboli from prostate cancer. Furthermore, histology revealed differences in the androgen receptors in the prostate and emboli, with significantly greater Ki-67 expression in the emboli than in the prostate.
Conclusion: Prostate cancer proliferated in the pulmonary artery after hematogenous metastasis, caused vascular occlusion, and formed microscopic pulmonary tumor embolisms.
Keywords: androgen receptor; cadherin; microscopic pulmonary tumor embolism; prostate cancer; pulmonary hypertension.
© 2020 The Authors. IJU Case Reports published by John Wiley & Sons Australia, Ltd on behalf of the Japanese Urological Association.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Microscopic pulmonary tumor embolism secondary to adenocarcinoma of the prostate.Hinyokika Kiyo. 2003 Mar;49(3):169-72. Hinyokika Kiyo. 2003. PMID: 12728533 Review.
-
An Autopsy Case of Pulmonary Tumor Emboli Due to Metastatic Squamous Cell Carcinoma.Cureus. 2021 Nov 12;13(11):e19506. doi: 10.7759/cureus.19506. eCollection 2021 Nov. Cureus. 2021. PMID: 34912643 Free PMC article.
-
[Pulmonary microscopic tumor embolism syndrome].Dtsch Med Wochenschr. 2006 Mar 24;131(12):618-21. doi: 10.1055/s-2006-933704. Dtsch Med Wochenschr. 2006. PMID: 16544237 German.
-
[A case of microscopic pulmonary tumor emboli 14 months after total cystectomy].Hinyokika Kiyo. 2004 Apr;50(4):279-81. Hinyokika Kiyo. 2004. PMID: 15188624 Japanese.
-
Pulmonary tumor thrombotic microangiopathy: the challenge of the antemortem diagnosis.J Cardiovasc Med (Hagerstown). 2014 Nov;15(11):828-33. doi: 10.2459/JCM.0b013e328354e473. J Cardiovasc Med (Hagerstown). 2014. PMID: 22710763 Review.
Cited by
-
Editorial Comment to Microscopic pulmonary tumor embolism from adenocarcinoma of the prostate.IJU Case Rep. 2020 May 16;3(5):165. doi: 10.1002/iju5.12164. eCollection 2020 Sep. IJU Case Rep. 2020. PMID: 32914060 Free PMC article. No abstract available.
-
Tumor embolism and acute arterial occlusion: A systematic review.Surg Open Sci. 2022 Nov 7;10:216-222. doi: 10.1016/j.sopen.2022.10.006. eCollection 2022 Oct. Surg Open Sci. 2022. PMID: 36389271 Free PMC article. Review.
-
Pulmonary tumor embolism: A retrospective study over a 30-year period.PLoS One. 2021 Aug 11;16(8):e0255917. doi: 10.1371/journal.pone.0255917. eCollection 2021. PLoS One. 2021. PMID: 34379693 Free PMC article.
References
-
- Kane RD, Hawkins HK, Miller JA, Noce PS. Pulmonary tumor emboli. Cancer 1975; 36: 1473–82. - PubMed
-
- Miedema EB, Redman JF. Microscopic pulmonary embolization by adenocarcinoma of prostate. Urology 1981; 18: 399–401. - PubMed
-
- Keeping IM, Buchanan R, Dadds JH. Microscopic pulmonary emboli from carcinoma of the prostate. Br. J. Dis. Chest. 1982; 76: 298–300. - PubMed
-
- Nakano M, Miwa K, Kanimoto Y, Ishihara S, Deguchi T. Microscopic pulmonary tumor embolism secondary to adenocarcinoma of the prostate. Acta Urol. Jpn 2003; 49: 169–72. - PubMed
-
- Mainardi AS, Trow T. Tumor emboli. A rare cause of acute pulmonary hypertension. Am. J. Med. 2016; 4: e137–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources