

Positive end-expiratory pressure-induced recruited lung volume measured by volume-pressure curves in acute respiratory distress syndrome: a physiologic systematic review and meta-analysis
- PMID: 32915255
- PMCID: PMC7484614
- DOI: 10.1007/s00134-020-06226-9
Positive end-expiratory pressure-induced recruited lung volume measured by volume-pressure curves in acute respiratory distress syndrome: a physiologic systematic review and meta-analysis
Abstract
Purpose: Recruitment of lung volume is often cited as the reason for using positive end-expiratory pressure (PEEP) in acute respiratory distress syndrome (ARDS) patients. We performed a systematic review on PEEP-induced recruited lung volume measured from inspiratory volume-pressure (VP) curves in ARDS patients to assess the prevalence of patients with PEEP-induced recruited lung volume and the mortality in recruiters and non-recruiters.
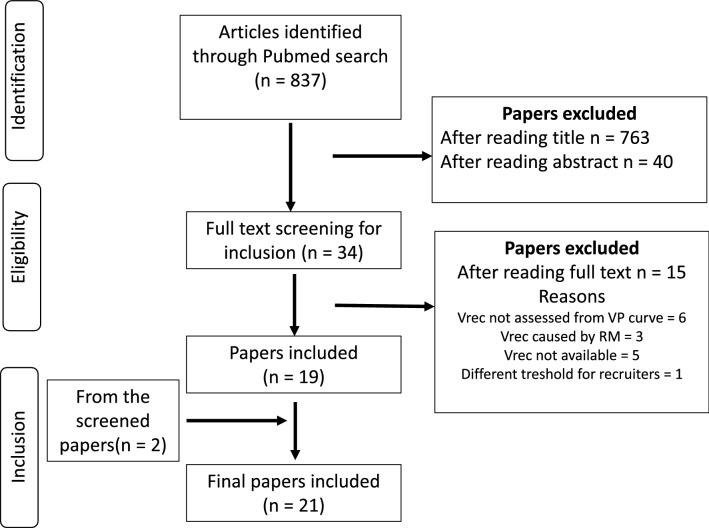
Methods: We conducted a systematic search of PubMed to identify studies including ARDS patients in which the intervention of an increase in PEEP was accompanied by measurement of the recruited volume (Vrec increase versus no increase) using the VP curve in order to assess the relation between Vrec and mortality at ICU discharge. We first analysed the pooled data from the papers identified and then analysed individual patient level data received from the authors via personal contact. The risk of bias of the included papers was assessed using the quality in prognosis studies tool and the certainty of the evidence regarding the relationship of mortality to Vrec by the GRADE approach. Recruiters were defined as patients with a Vrec > 150 ml. A random effects model was used for the pooled data. Multivariable logistic regression analysis was used for individual patient data.
Results: We identified 16 papers with a total of 308 patients for the pooled data meta-analysis and 14 papers with a total of 384 patients for the individual data analysis. The quality of the articles was moderate. In the pooled data, the prevalence of recruiters was 74% and the mortality was not significantly different between recruiters and non-recruiters (relative risk 1.20 [95% confidence intervals 0.88-1.63]). The certainty of the evidence regarding this association was very low and publication bias evident. In the individual data, the prevalence of recruiters was 70%. In the multivariable logistic regression, Vrec was not associated with mortality but Simplified Acute Physiology Score II and driving pressure at PEEP of 5 cmH2O were.
Conclusion: After a PEEP increment, most patients are recruiters. Vrec was not associated with ICU mortality. The presence of similar findings in the individual patient level analysis and the driving pressure at PEEP of 5 cmH2O was associated with mortality as previously reported validate our findings. Publication bias and the lack of prospective studies suggest more research is required.
Keywords: Alveolar recruitment; Lung recruitment; Positive end-expiratory pressure; Positive-pressure respiration/therapeutic use; Respiratory distress syndrome, adult/mortality; Respiratory distress syndrome, adult/physiopathology; Respiratory distress syndrome, adult/therapy.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures





References
-
- Grasso S, Mascia L, Del Turco M, Malacarne P, Giunta F, Brochard L, Slutsky AS, Marco Ranieri V. Effects of recruiting maneuvers in patients with acute respiratory distress syndrome ventilated with protective ventilatory strategy. Anesthesiology. 2002;96:795–802. doi: 10.1097/00000542-200204000-00005. - DOI - PubMed
-
- Iorio A, Spencer FA, Falavigna M, Alba C, Lang E, Burnand B, McGinn T, Hayden J, Williams K, Shea B, Wolff R, Kujpers T, Perel P, Vandvik PO, Glasziou P, Schunemann H, Guyatt G. Use of GRADE for assessment of evidence about prognosis: rating confidence in estimates of event rates in broad categories of patients. BMJ. 2015;350:h870. doi: 10.1136/bmj.h870. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
