

Cavernous transformation of the portal vein in pancreatic cancer surgery-venous bypass graft first
- PMID: 32915294
- PMCID: PMC7541372
- DOI: 10.1007/s00423-020-01974-0
Cavernous transformation of the portal vein in pancreatic cancer surgery-venous bypass graft first
Abstract
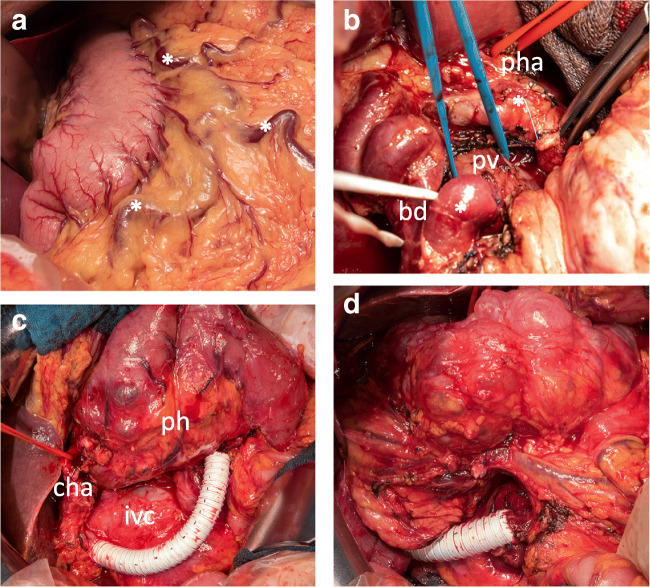
Background: In recent years, several techniques have been introduced to allow safe oncologic resections of cancers of the pancreatic head. While resections of the mesenterico-portal axis became now a part of the routine treatment, patients with a cavernous transformation of the portal vein still pose a surgical challenge and are regularly deemed unresectable.
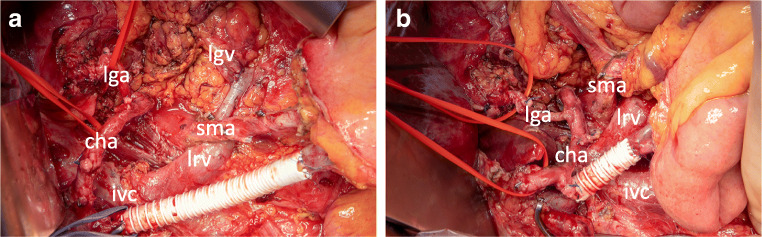
Objective: Here, we describe a technique of initial venous bypass graft placement between the superior mesenteric vein or its tributaries and the portal vein before the resection of the pancreatic head. This approach avoids uncontrollable bleeding as well as venous congestion of the intestine with a continuous hepatic perfusion and facilitates oncologic resection of pancreatic head cancers. This technique, in combination with previously published resection strategies, enables tumor resection in locally advanced pancreatic head cancers.
Conclusions: Venous bypass graft first operations facilitate and enable the resection of the pancreatic head cancers in patients with a cavernous transformation of the portal vein thus rendering these patients resectable.
Keywords: Cavernous transformation; Pancreatic cancer; Surgery; Venous bypass graft.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Klaiber U, Schnaidt ES, Hinz U, Gaida MM, Heger U, Hank T, Strobel O, Neoptolemos JP, Mihaljevic AL, Buchler MW, Hackert T (2019) Prognostic factors of survival after neoadjuvant treatment and resection for initially unresectable pancreatic cancer. Ann Surg. 10.1097/SLA.0000000000003270 - PubMed
-
- Murphy JE, Wo JY, Ryan DP, Jiang W, Yeap BY, Drapek LC, Blaszkowsky LS, Kwak EL, Allen JN, Clark JW, Faris JE, Zhu AX, Goyal L, Lillemoe KD, DeLaney TF, Fernandez-Del Castillo C, Ferrone CR, Hong TS. Total neoadjuvant therapy with FOLFIRINOX followed by individualized chemoradiotherapy for borderline resectable pancreatic adenocarcinoma: a phase 2 clinical trial. JAMA Oncol. 2018;4(7):963–969. doi: 10.1001/jamaoncol.2018.0329. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
