

Derivation and validation of the J-CTO extension score for pre-procedural prediction of major adverse cardiac and cerebrovascular events in patients with chronic total occlusions
- PMID: 32915843
- PMCID: PMC7485776
- DOI: 10.1371/journal.pone.0238640
Derivation and validation of the J-CTO extension score for pre-procedural prediction of major adverse cardiac and cerebrovascular events in patients with chronic total occlusions
Abstract
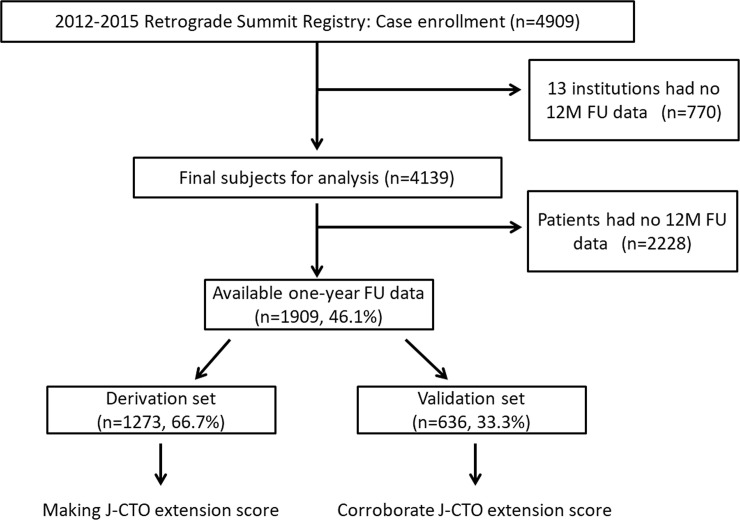
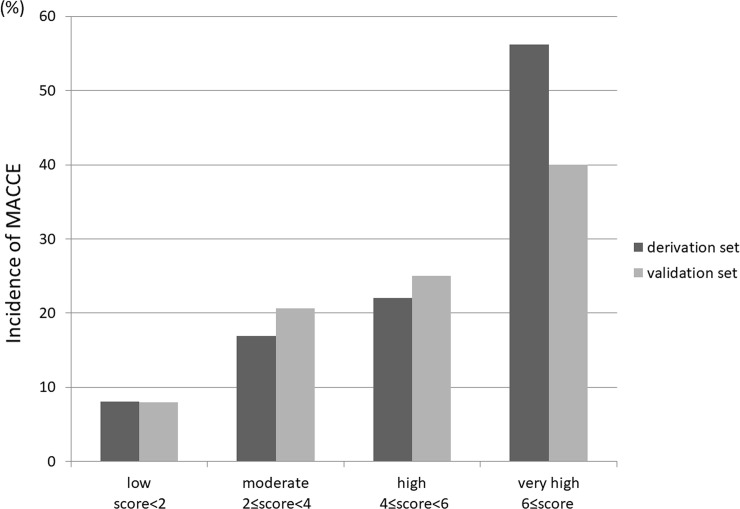
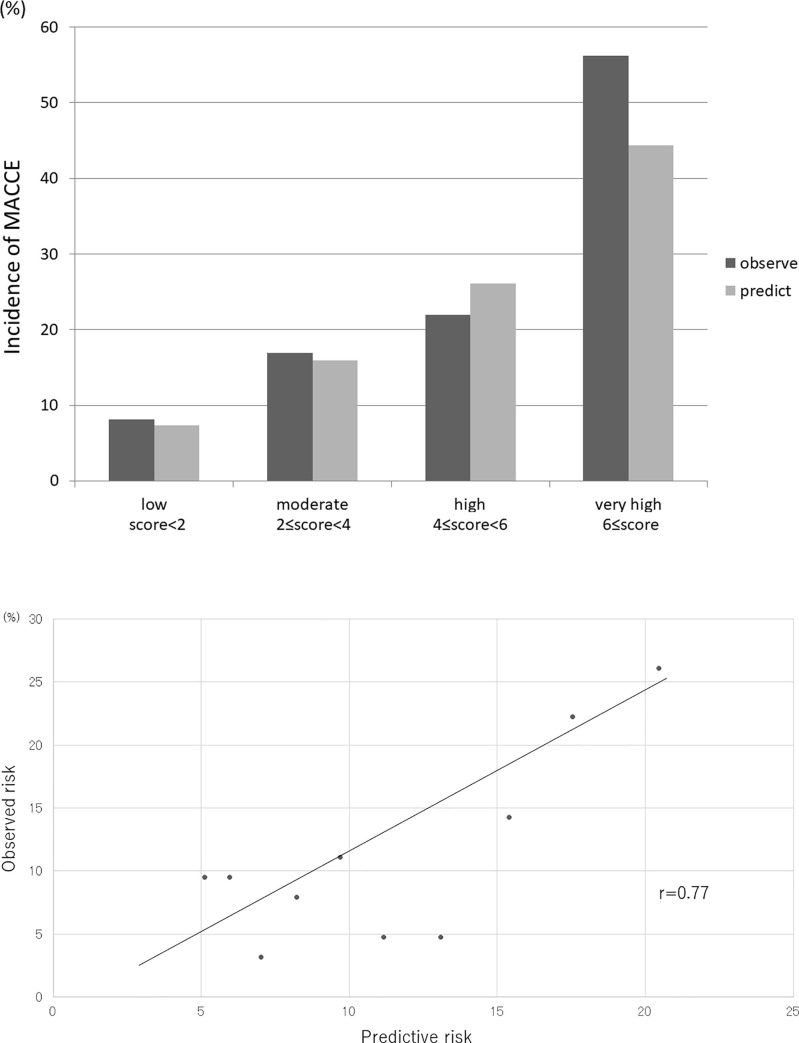
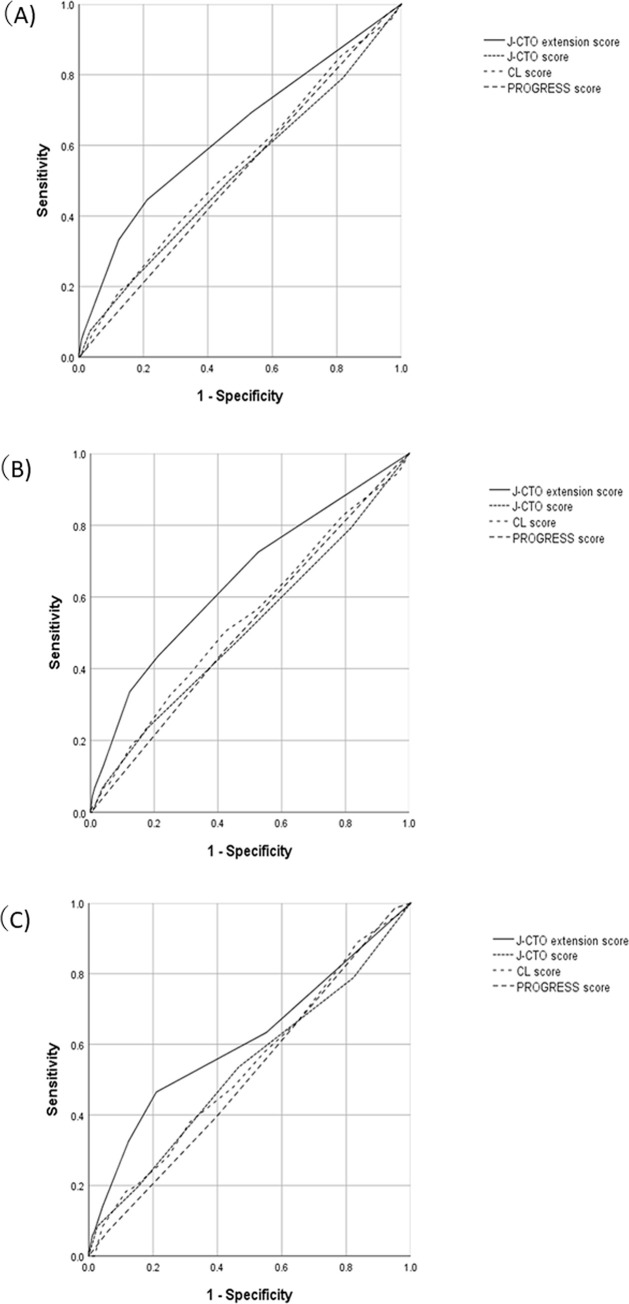
We developed a prediction model of long-term risk after percutaneous coronary intervention (PCI) for coronary chronic total occlusion (CTO) based on pre-procedural clinical information. A total of 4,139 eligible patients, who underwent CTO-PCI at 52 Japanese centers were included. Specifically, 1,909 patients with 1-year data were randomly divided into the derivation (n = 1,273) and validation (n = 636) groups. Major adverse cardiac and cardiovascular event (MACCE) was the primary endpoint, including death, stroke, revascularization, and non-fatal myocardial infarction. We assessed the performance of our model using the area under the receiver operating characteristic curve (AUC) and assigned a simplified point-scoring system. One-hundred-thirty-eight (10.8%) patients experienced MACCE in the derivation cohort with hemodialysis (HD: odds ratio [OR] = 2.55), left ventricular ejection fractions (LVEF) <35% (OR = 2.23), in-stent occlusions (ISO: OR = 2.27), and diabetes mellitus (DM: OR = 1.72). The AUC of the derivation model was 0.650. The model's performance was similar in the validation cohort (AUC, 0.610). When assigned a point for each associated factor (HD = 3, LVEF <35%, ISO = 2, and DM = 1 point), the average predicted versus the observed MACCE probability using the Japan-CTO extension score for the low, moderate, high, and very high risk groups was 8.1% vs. 7.3%, 16.9% vs. 15.9%, 22.0% vs. 26.1%, and 56.2% vs. 44.4%, respectively. This novel risk model may allow for the estimation of long-term risk and be useful in disseminating appropriate revascularization procedures.
Conflict of interest statement
Soichiro Ebisawa belongs to Endowed Department of Cardiovascular Medicine of Shinshu University supported by Medtronic Japan Co.,Ltd. Abbott Vascular Japan Co.,Ltd. Boston Scientific Japan, TERUMO CORPORATION, Cardinal Health Japan and NIPRO CORPORATION. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Teeuwen K, van der Schaaf RJ, Adriaenssens T, Koolen JJ, Smits PC, Henriques JPS, et al. Randomized multicenter trial investigating angiographic outcomes of hybrid sirolimus-eluting stents with biodegradable polymer compared with everolimus-eluting stents with durable polymer in chronic total occlusions: The PRISON IV trial. JACC Cardiovasc Interv. 2017;10:133–143. - PubMed
-
- Prasad A, Rihal CS, Lennon RJ, Wiste HJ, Singh M, Holmes DR Jr. Trends in outcomes after percutaneous coronary intervention for chronic total occlusions: a 25-year experience from the Mayo Clinic. J Am Coll Cardiol. 2007;49:1611–1618. - PubMed
-
- Kato M, Kimura T, Morimoto T, Nishikawa H, Uchida F, Suzuki H, et al. Comparison of five-year outcome of sirolimus-eluting stent implantation for chronic total occlusions versus for non-chronic total occlusion (from the j-Cypher registry). Am J Cardiol. 2012;110:1282–1289. - PubMed
-
- Maeremans J, Dens J, Spratt JC Bagnall AJ, Stuijfzand W, Nap A, et al. Recharge investigators. antegrade dissection and reentry as part of the hybrid chronic total occlusion revascularization strategy: a subanalysis of the RECHARGE Registry (Registry of CrossBoss and Hybrid Procedures in France, the Netherlands, Belgium and United Kingdom). Circ Cardiovasc Interv. 2017;10:e004791. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
