

Favourable long-term survival of patients with esophageal cancer treated with extended transhiatal esophagectomy combined with en bloc lymphadenectomy: results from a retrospective observational cohort study
- PMID: 32917177
- PMCID: PMC7488573
- DOI: 10.1186/s12893-020-00855-z
Favourable long-term survival of patients with esophageal cancer treated with extended transhiatal esophagectomy combined with en bloc lymphadenectomy: results from a retrospective observational cohort study
Abstract
Background: Although considered complex and challenging, esophagectomy remains the best potentially curable treatment option for resectable esophageal and esophagogastric junction (AEG) carcinomas. The optimal surgical approach and technique as well as the extent of lymphadenectomy, particularly regarding quality of life and short- and long-term outcomes, are still a matter of debate. To lower perioperative morbidity, we combined the advantages of a one-cavity approach with extended lymph node dissection (usually achieved by only a two-cavity approach) and developed a modified single-cavity transhiatal approach for esophagectomy.
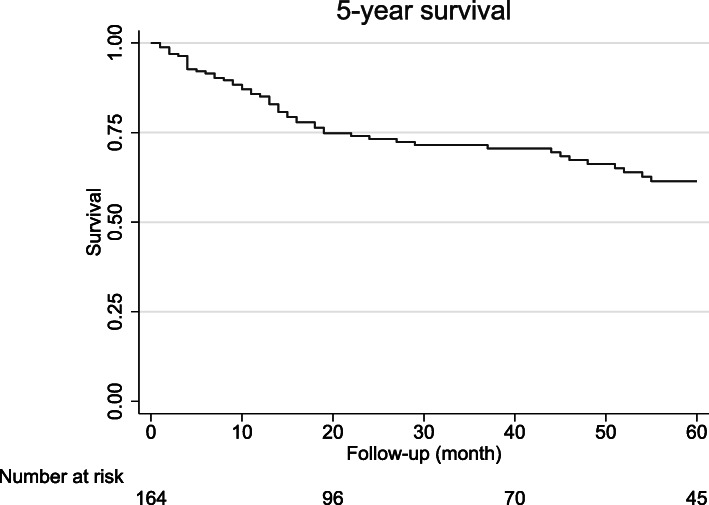
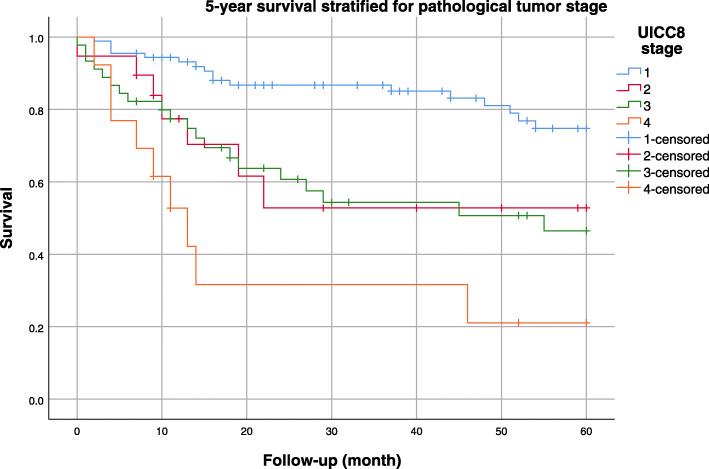
Methods: The aim of this study was to evaluate the outcome of an extended transhiatal esophageal resection with radical bilateral mediastinal en bloc lymphadenectomy (eTHE). A prospective database of 166 patients with resectable cancers of the esophagus (including adenocarcinomas of the AEG types I and II) were analyzed. Patients were treated between 2001 and 2017 with eTHE at a tertiary care university center. Relevant patient characteristics and outcome parameters were collected and analyzed. The primary endpoint was 5-year overall survival. Secondary outcomes included short-term morbidity, mortality, radicalness of en bloc resection and oncologic efficacy.
Results: The overall survival rates at 1, 3 and 5 years were 84, 70, and 61.0%, respectively. The in-hospital mortality rate after eTHE was 1.2%. Complications with a Clavien-Dindo score of III/IV occurred in 31 cases (18.6%). A total of 25 patients (15.1%) had a major pulmonary complication. The median hospital stay was 17 days (interquartile range (IQR) 12). Most patients (n = 144; 86.7%) received neoadjuvant treatment. The median number of lymph nodes resected was 25 (IQR 17). The R0 resection rate was 97%.
Conclusion: In patients with esophageal cancer, eTHE without thoracotomy resulted in excellent long-term survival, an above average number of resected lymph nodes and an acceptable postoperative morbidity and mortality.
Keywords: En bloc lymphadenectomy; Esophageal cancer; Extended transhiatal esophagectomy; Long-term survival; Short-term outcome.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Perioperative outcomes of single-port mediastinoscope-assisted transhiatal esophagectomy for thoracic esophageal cancer.Dis Esophagus. 2017 Oct 1;30(10):1-8. doi: 10.1093/dote/dox047. Dis Esophagus. 2017. PMID: 28859387
-
The CARDIA-trial protocol: a multinational, prospective, randomized, clinical trial comparing transthoracic esophagectomy with transhiatal extended gastrectomy in adenocarcinoma of the gastroesophageal junction (GEJ) type II.BMC Cancer. 2020 Aug 20;20(1):781. doi: 10.1186/s12885-020-07152-1. BMC Cancer. 2020. PMID: 32819399 Free PMC article.
-
Evidence-based selective application of transhiatal esophagectomy in a high-volume esophageal center.World J Surg. 2012 Jan;36(1):98-103. doi: 10.1007/s00268-011-1307-0. World J Surg. 2012. PMID: 21979584
-
Transhiatal esophagectomy.Surg Clin North Am. 2005 Jun;85(3):593-610. doi: 10.1016/j.suc.2005.01.009. Surg Clin North Am. 2005. PMID: 15927654 Review.
-
Laparoscopic transhiatal esophagectomy for esophageal cancer.Am J Surg. 2005 Jul;190(1):69-74. doi: 10.1016/j.amjsurg.2004.12.004. Am J Surg. 2005. PMID: 15972176 Review.
Cited by
-
Application of Amiodarone and Cedilan in the Treatment of Patients with Arrhythmia after Esophageal and Lung Cancer.Evid Based Complement Alternat Med. 2023 Apr 13;2023:8026918. doi: 10.1155/2023/8026918. eCollection 2023. Evid Based Complement Alternat Med. 2023. Retraction in: Evid Based Complement Alternat Med. 2023 Dec 6;2023:9876708. doi: 10.1155/2023/9876708. PMID: 37089714 Free PMC article. Retracted.
-
Long-Term, Health-Related Quality of Life after Open and Robot-Assisted Ivor-Lewis Procedures-A Propensity Score-Matched Study.J Clin Med. 2020 Oct 30;9(11):3513. doi: 10.3390/jcm9113513. J Clin Med. 2020. PMID: 33142987 Free PMC article.
-
Engineered Full Thickness Electrospun Scaffold for Esophageal Tissue Regeneration: From In Vitro to In Vivo Approach.Pharmaceutics. 2022 Jan 21;14(2):252. doi: 10.3390/pharmaceutics14020252. Pharmaceutics. 2022. PMID: 35213985 Free PMC article.
-
Long-Term Outcomes of Colon Conduits in Surgery for Primary Esophageal Cancer: A Propensity Score-Matched Comparison to Gastric Conduits.J Chest Surg. 2024 Jan 5;57(1):53-61. doi: 10.5090/jcs.23.074. J Chest Surg. 2024. PMID: 38174891 Free PMC article.
-
A Nomogram Model to Predict Post-Progression Survival in Esophageal Squamous Cell Carcinoma Patients With Recurrence After Radical Resection.Front Oncol. 2022 Jul 7;12:925685. doi: 10.3389/fonc.2022.925685. eCollection 2022. Front Oncol. 2022. PMID: 35875105 Free PMC article.
References
-
- Biere SS, van Berge Henegouwen MI, Maas KW, Bonavina L, Rosman C, Garcia JR, et al. Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomised controlled trial. Lancet. 2012;379(9829):1887–1892. doi: 10.1016/S0140-6736(12)60516-9. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
