

Radiomics Improves Cancer Screening and Early Detection
- PMID: 32917666
- PMCID: PMC12306495
- DOI: 10.1158/1055-9965.EPI-20-0075
Radiomics Improves Cancer Screening and Early Detection
Abstract
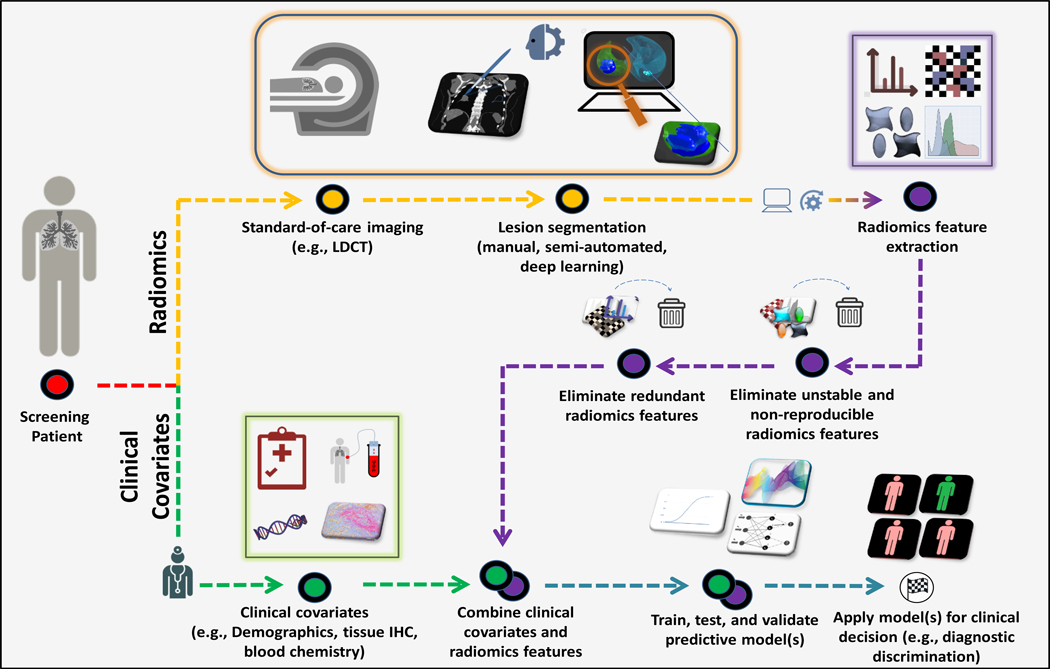
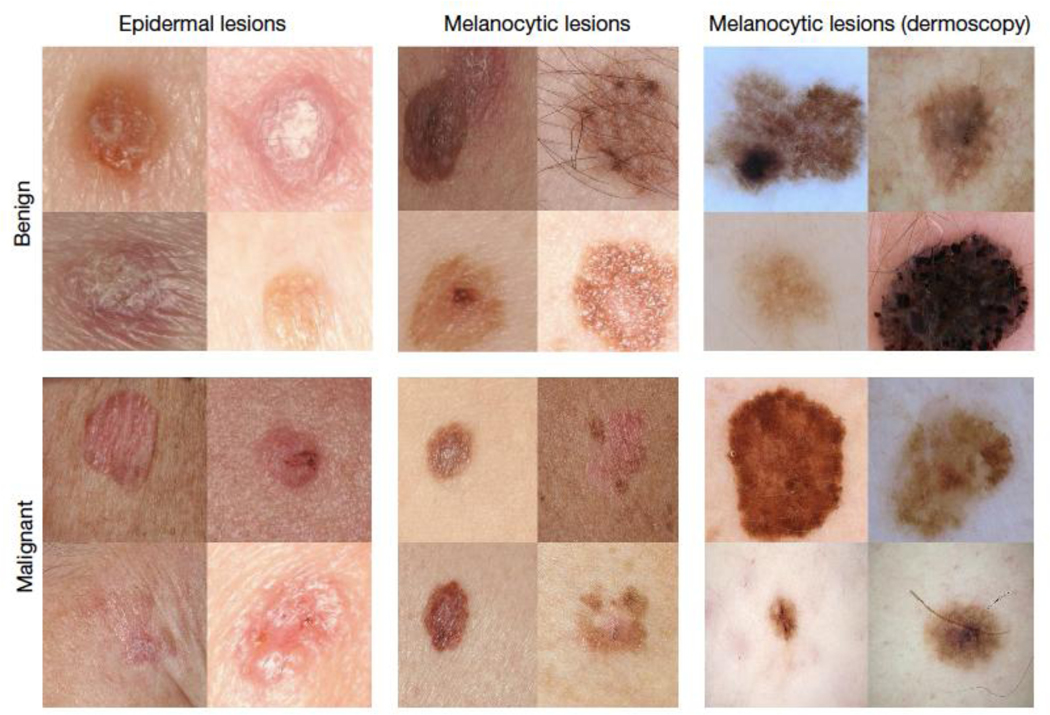
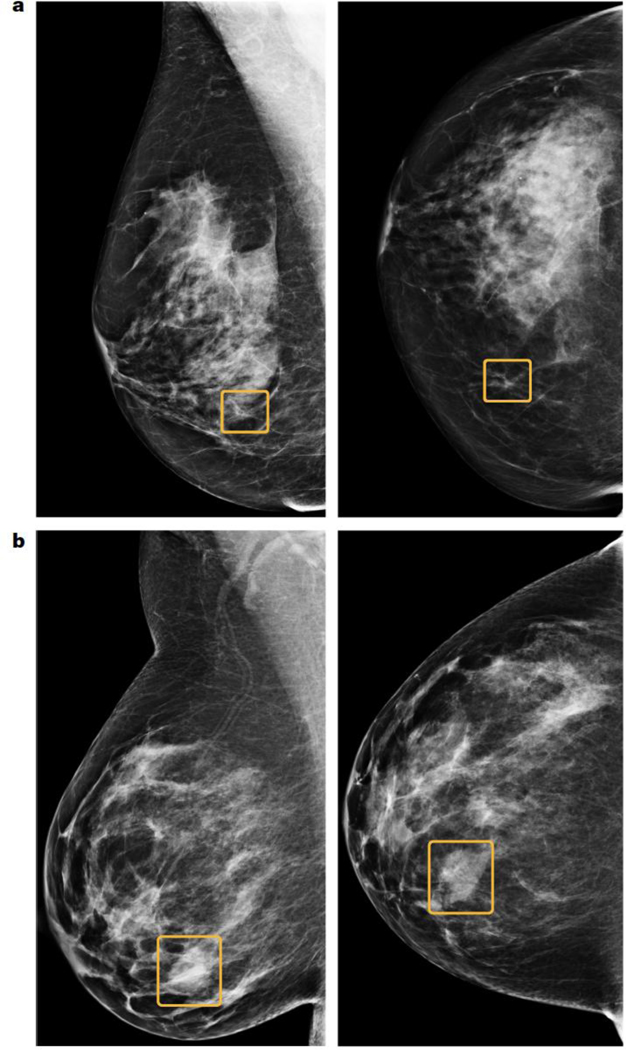
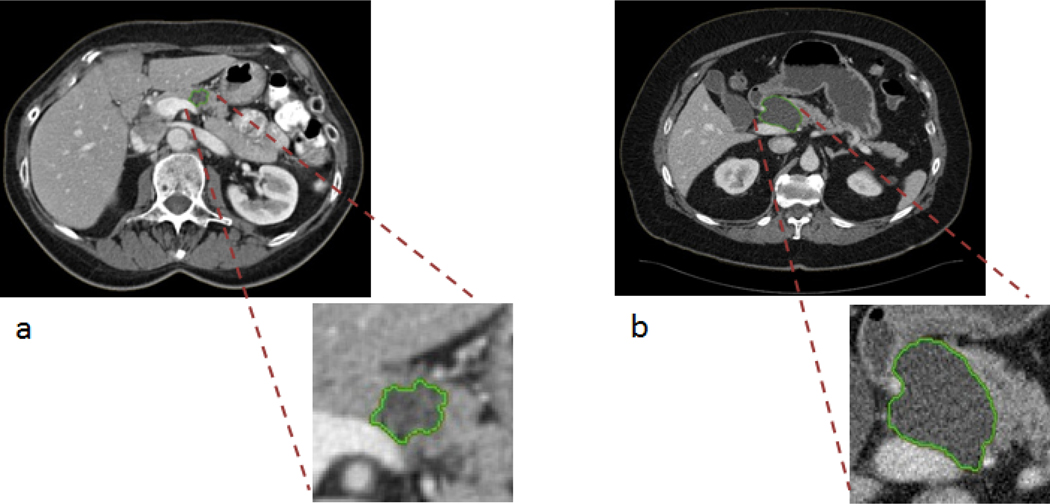
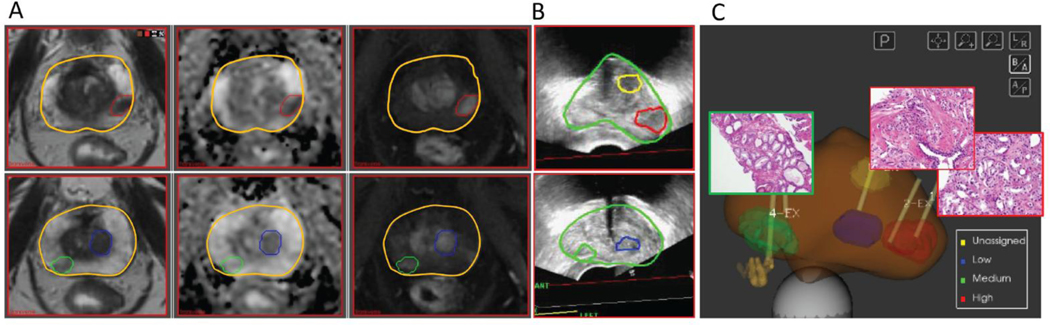
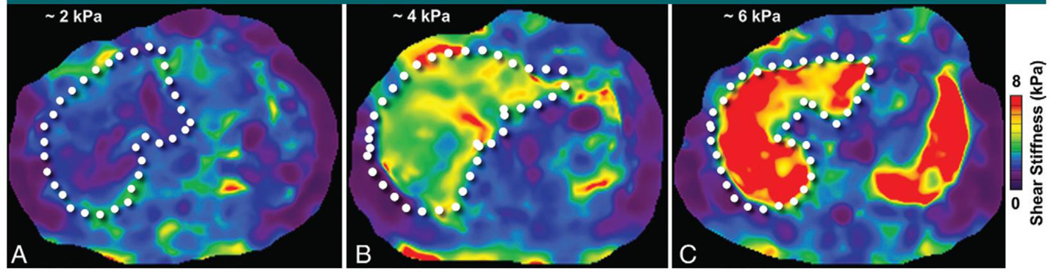
Imaging is a key technology in the early detection of cancers, including X-ray mammography, low-dose CT for lung cancer, or optical imaging for skin, esophageal, or colorectal cancers. Historically, imaging information in early detection schema was assessed qualitatively. However, the last decade has seen increased development of computerized tools that convert images into quantitative mineable data (radiomics), and their subsequent analyses with artificial intelligence (AI). These tools are improving diagnostic accuracy of early lesions to define risk and classify malignant/aggressive from benign/indolent disease. The first section of this review will briefly describe the various imaging modalities and their use as primary or secondary screens in an early detection pipeline. The second section will describe specific use cases to illustrate the breadth of imaging modalities as well as the benefits of quantitative image analytics. These will include optical (skin cancer), X-ray CT (pancreatic and lung cancer), X-ray mammography (breast cancer), multiparametric MRI (breast and prostate cancer), PET (pancreatic cancer), and ultrasound elastography (liver cancer). Finally, we will discuss the inexorable improvements in radiomics to build more robust classifier models and the significant limitations to this development, including access to well-annotated databases, and biological descriptors of the imaged feature data.See all articles in this CEBP Focus section, "NCI Early Detection Research Network: Making Cancer Detection Possible."
©2020 American Association for Cancer Research.
Conflict of interest statement
No potential conflicts of interest were disclosed by M.B.S.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
