

Physicians' very brief (30-sec) intervention for smoking cessation on 13 671 smokers in China: a pragmatic randomized controlled trial
- PMID: 32918512
- PMCID: PMC8246886
- DOI: 10.1111/add.15262
Physicians' very brief (30-sec) intervention for smoking cessation on 13 671 smokers in China: a pragmatic randomized controlled trial
Abstract
Background and aims: Three to 10 minutes of smoking cessation advice by physicians is effective to increase quit rates, but is not routinely practised. We examined the effectiveness of physicians' very brief (approximately 30 sec) smoking cessation intervention on quit rates among Chinese outpatient smokers.
Design: A pragmatic, open-label, individually randomized controlled trial.
Setting: Seventy-two medical outpatient departments of hospitals and/or community health centers in Guangdong, China.
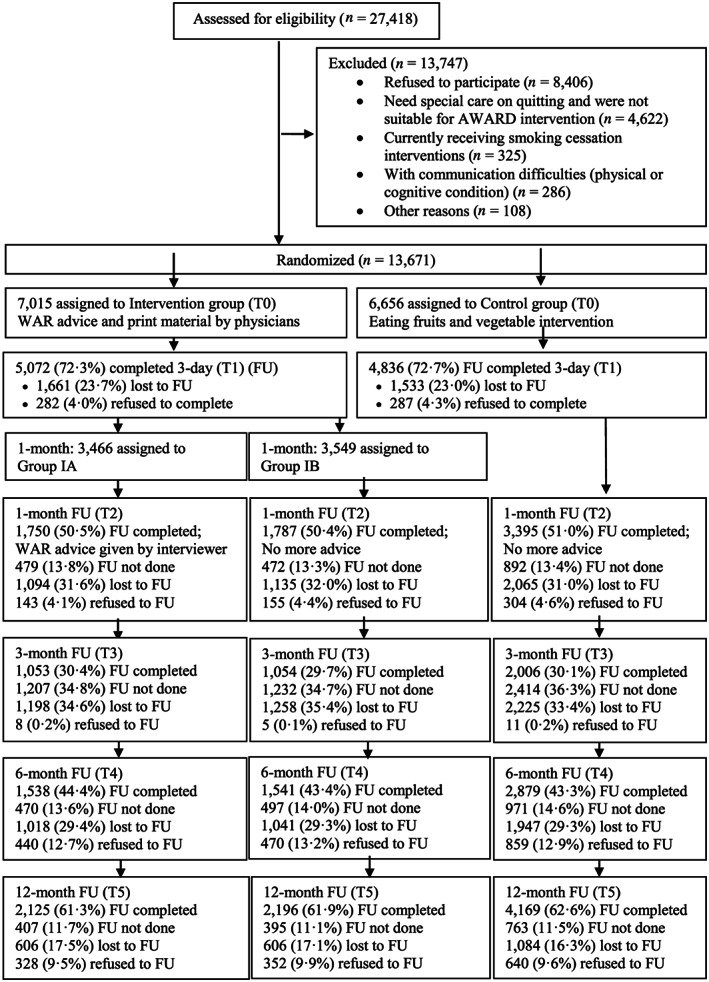
Participants: Chinese adults who were daily cigarette smokers (n = 13 671, 99% males) were invited by their physician to participate during outpatient consultation. Smokers who were receiving smoking cessation treatment or were judged to need specialist treatment for cessation were excluded.
Interventions: The intervention group (n = 7015) received a 30-sec intervention including physician's very brief advice, a leaflet with graphic warnings and a card with contact information of available cessation services. The control group (n = 6656) received a very brief intervention on consuming vegetables and fruit. A total of 3466 participants in the intervention group were further randomized to receive a brief booster advice from trained study personnel via telephone 1 month following their doctor visit.
Measurements: The primary outcome was self-reported 7-day point prevalence abstinence (PPA) in the intervention and control groups at the 12-month follow-up. Secondary outcomes included self-reported 30-day abstinence and biochemically validated abstinence at 12-month follow-up.
Findings: By intention-to-treat, the intervention (versus control) group had greater self-reported 7-day abstinence [9.1 versus 7.8%, odds ratio (OR) = 1.14, 95% confidence interval (CI) = 1.03-1.26, P = 0.008] and 30-day abstinence (8.0 versus 6.9%, OR = 1.14, 95% CI = 1.03-1.27, P = 0.01) at 12-month follow-up. The effect size increased when only participants who received the intervention from compliant physicians were included (7-day PPA, OR = 1.42, 95% CI = 1.11-1.74). The group difference in biochemically validated abstinence was small (0.8 versus 0.8%, OR = 1.00, 95% CI = 0.71-1.42, P = 0.99).
Conclusion: A 30-sec smoking cessation intervention increased self-reported abstinence among mainly male smokers in China at 12-month follow-up (risk difference = 1.3%), and should be feasible to provide in most settings and delivered by all health-care professionals.
Keywords: Physicians; RCT; Tobacco; pragmatic; smoking cessation; very brief intervention.
© 2020 The Authors. Addiction published by John Wiley & Sons Ltd on behalf of Society for the Study of Addiction.
Figures
References
-
- Forouzanfar M. H., Alexander L., Anderson H. R., Bachman V. F., Biryukov S., Brauer M., et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: a systematic analysis for the global burden of disease study 2013. Lancet 2015; 386: 2287–2323. - PMC - PubMed
-
- Gakidou E., Afshin A., Abajobir A. A., Abate K. H., Abbafati C., Abbas K. M., et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet 2017; 390: 1345–1422. - PMC - PubMed
-
- World Health Organization (WHO) A Guide for Tobacco Users to Quit. Geneva: WHO; 2014.
-
- Lam T. H. Absolute risk of tobacco deaths: one in two smokers will be killed by smoking: comment on ‘smoking and all‐cause mortality in older people’. Arch Intern Med 2012; 172: 845–846. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
