

The misdiagnosis of prolonged disorders of consciousness by a clinical consensus compared with repeated coma-recovery scale-revised assessment
- PMID: 32919461
- PMCID: PMC7488705
- DOI: 10.1186/s12883-020-01924-9
The misdiagnosis of prolonged disorders of consciousness by a clinical consensus compared with repeated coma-recovery scale-revised assessment
Abstract
Background: Previous studies have shown that a single Coma-Recovery Scale-Revision (CRS-R) assessment can identify high rates of misdiagnosis by clinical consensus. The aim of this study was to investigate the proportion of misdiagnosis by clinical consensus compared to repeated behavior-scale assessments in patients with prolonged disorders of consciousness (DOC).
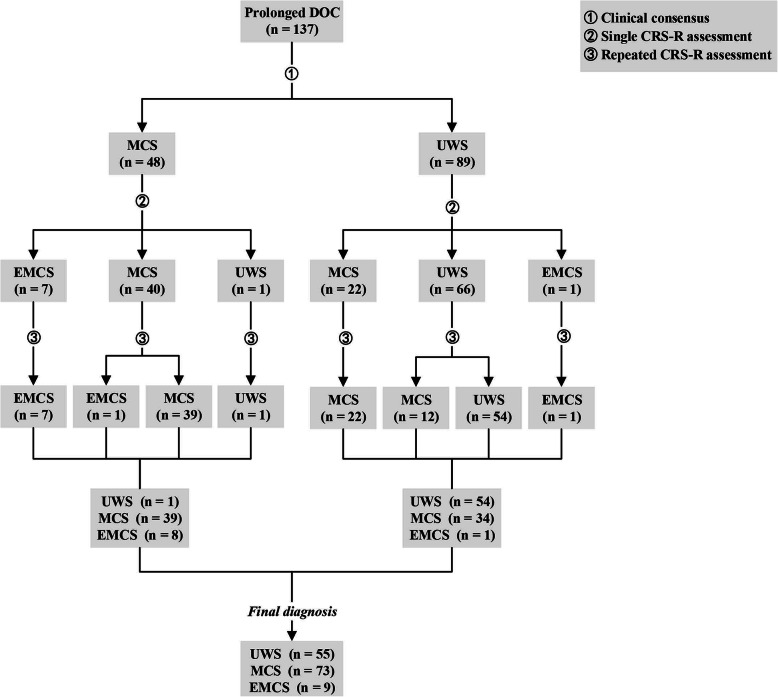
Methods: Patients with prolonged DOC during hospitalization were screened by clinicians, and the clinicians formed a clinical-consensus diagnosis. Trained professionals used the CRS-R to evaluate the consciousness levels of the enrolled patients repeatedly (≥5 times) within a week. Based on the repeated evaluation results, the enrolled patients with prolonged DOC were divided into unresponsive wakefulness syndrome (UWS), minimally conscious state (MCS), and emergence from MCS (EMCS). Finally, the relationship between the results of the CRS-R and the clinical consensus were analyzed.
Results: In this study, 137 patients with a clinical-consensus diagnosis of prolonged DOC were enrolled. It was found that 24.7% of patients with clinical UWS were actually in MCS after a single CRS-R behavior evaluation, while the repeated CRS-R evaluation results showed that the proportion of misdiagnosis of MCS was 38.2%. A total of 16.7% of EMCS patients were misdiagnosed with clinical MCS, and 1.1% of EMCS patients were misdiagnosed with clinical UWS.
Conclusions: The rate of the misdiagnosis by clinical consensus is still relatively high. Therefore, clinicians should be aware of the importance of the bedside CRS-R behavior assessment and should apply the CRS-R tool in daily procedures.
Trial registration: ClinicalTrials.gov ID: NCT04139239 ; Registered 24 October 2019 - Retrospectively registered.
Keywords: Coma-recovery scale-revised; Disorders of consciousness; Minimally conscious state; Misdiagnosis; Unresponsive wakefulness syndrome.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Bruno MA, Vanhaudenhuyse A, Thibaut A, Moonen G, Laureys S. From unresponsive wakefulness to minimally conscious PLUS and functional locked-in syndromes: recent advances in our understanding of disorders of consciousness. J Neurol. 2011;258(7):1373–1384. doi: 10.1007/s00415-011-6114-x. - DOI - PubMed
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
