

Circulating tumour DNA analysis to direct therapy in advanced breast cancer (plasmaMATCH): a multicentre, multicohort, phase 2a, platform trial
- PMID: 32919527
- PMCID: PMC7599319
- DOI: 10.1016/S1470-2045(20)30444-7
Circulating tumour DNA analysis to direct therapy in advanced breast cancer (plasmaMATCH): a multicentre, multicohort, phase 2a, platform trial
Abstract
Background: Circulating tumour DNA (ctDNA) testing might provide a current assessment of the genomic profile of advanced cancer, without the need to repeat tumour biopsy. We aimed to assess the accuracy of ctDNA testing in advanced breast cancer and the ability of ctDNA testing to select patients for mutation-directed therapy.
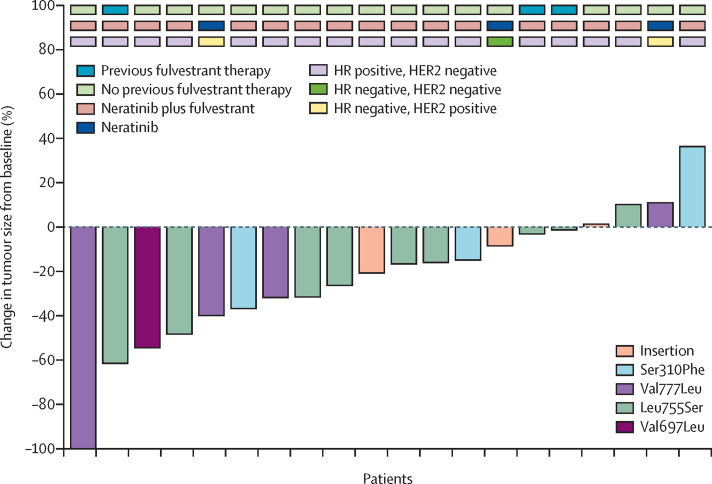
Methods: We did an open-label, multicohort, phase 2a, platform trial of ctDNA testing in 18 UK hospitals. Participants were women (aged ≥18 years) with histologically confirmed advanced breast cancer and an Eastern Cooperative Oncology Group performance status 0-2. Patients had completed at least one previous line of treatment for advanced breast cancer or relapsed within 12 months of neoadjuvant or adjuvant chemotherapy. Patients were recruited into four parallel treatment cohorts matched to mutations identified in ctDNA: cohort A comprised patients with ESR1 mutations (treated with intramuscular extended-dose fulvestrant 500 mg); cohort B comprised patients with HER2 mutations (treated with oral neratinib 240 mg, and if oestrogen receptor-positive with intramuscular standard-dose fulvestrant); cohort C comprised patients with AKT1 mutations and oestrogen receptor-positive cancer (treated with oral capivasertib 400 mg plus intramuscular standard-dose fulvestrant); and cohort D comprised patients with AKT1 mutations and oestrogen receptor-negative cancer or PTEN mutation (treated with oral capivasertib 480 mg). Each cohort had a primary endpoint of confirmed objective response rate. For cohort A, 13 or more responses among 78 evaluable patients were required to infer activity and three or more among 16 were required for cohorts B, C, and D. Recruitment to all cohorts is complete and long-term follow-up is ongoing. This trial is registered with ClinicalTrials.gov, NCT03182634; the European Clinical Trials database, EudraCT2015-003735-36; and the ISRCTN registry, ISRCTN16945804.
Findings: Between Dec 21, 2016, and April 26, 2019, 1051 patients registered for the study, with ctDNA results available for 1034 patients. Agreement between ctDNA digital PCR and targeted sequencing was 96-99% (n=800, kappa 0·89-0·93). Sensitivity of digital PCR ctDNA testing for mutations identified in tissue sequencing was 93% (95% CI 83-98) overall and 98% (87-100) with contemporaneous biopsies. In all cohorts, combined median follow-up was 14·4 months (IQR 7·0-23·7). Cohorts B and C met or exceeded the target number of responses, with five (25% [95% CI 9-49]) of 20 patients in cohort B and four (22% [6-48]) of 18 patients in cohort C having a response. Cohorts A and D did not reach the target number of responses, with six (8% [95% CI 3-17]) of 74 in cohort A and two (11% [1-33]) of 19 patients in cohort D having a response. The most common grade 3-4 adverse events were raised gamma-glutamyltransferase (13 [16%] of 80 patients; cohort A); diarrhoea (four [25%] of 20; cohort B); fatigue (four [22%] of 18; cohort C); and rash (five [26%] of 19; cohort D). 17 serious adverse reactions occurred in 11 patients, and there was one treatment-related death caused by grade 4 dyspnoea (in cohort C).
Interpretation: ctDNA testing offers accurate, rapid genotyping that enables the selection of mutation-directed therapies for patients with breast cancer, with sufficient clinical validity for adoption into routine clinical practice. Our results demonstrate clinically relevant activity of targeted therapies against rare HER2 and AKT1 mutations, confirming these mutations could be targetable for breast cancer treatment.
Funding: Cancer Research UK, AstraZeneca, and Puma Biotechnology.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures



Comment in
-
The future of liquid biopsy.Lancet Oncol. 2020 Dec;21(12):e550. doi: 10.1016/S1470-2045(20)30687-2. Lancet Oncol. 2020. PMID: 33271107 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
