

Preganglionic and Postganglionic Brachial Plexus Birth Injury Effects on Shoulder Muscle Growth
- PMID: 32919794
- PMCID: PMC7864858
- DOI: 10.1016/j.jhsa.2020.07.017
Preganglionic and Postganglionic Brachial Plexus Birth Injury Effects on Shoulder Muscle Growth
Abstract
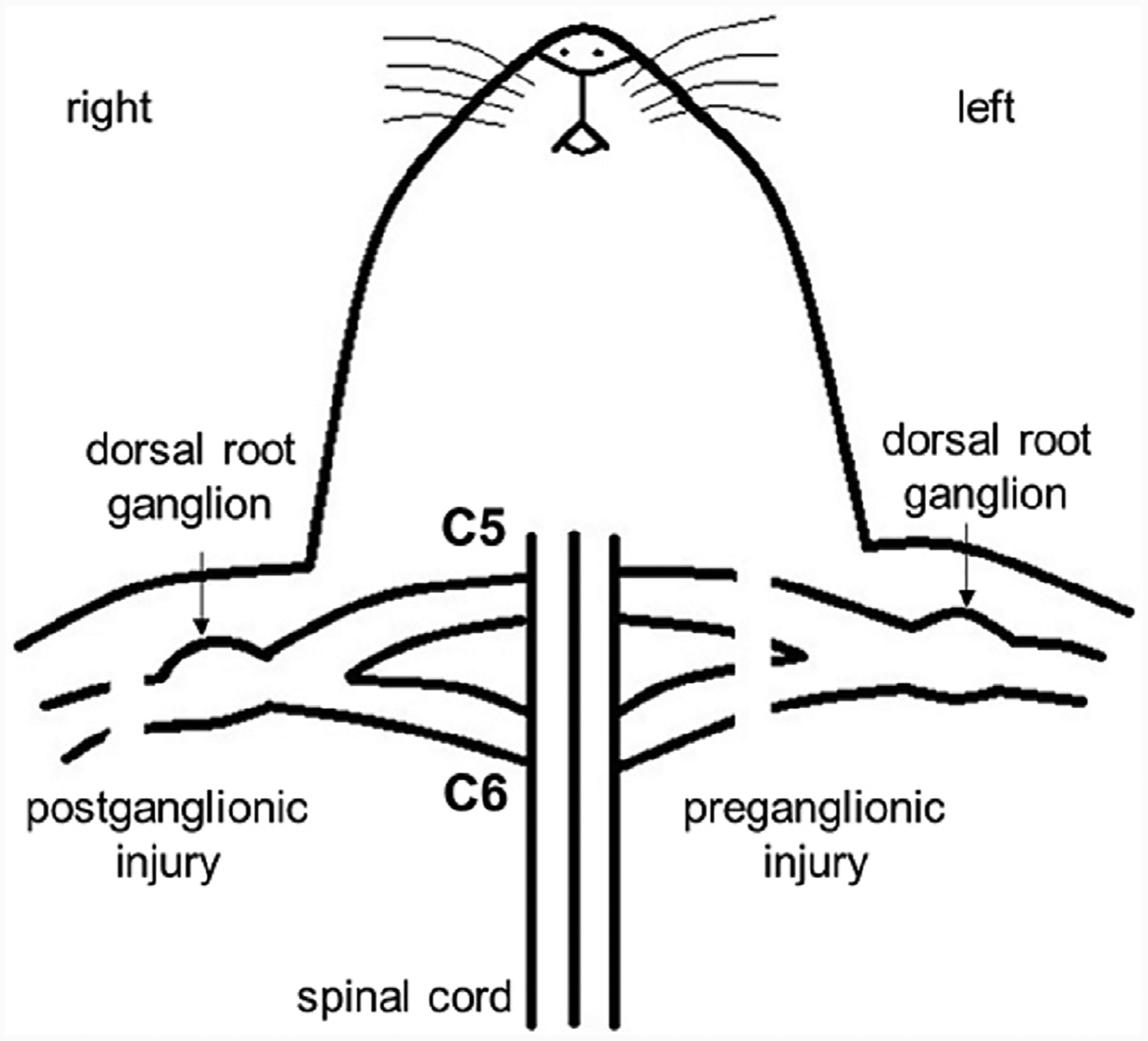
Purpose: Brachial plexus birth injury can differ in presentation, depending on whether the nerve ruptures distal to, or avulses proximal to, the dorsal root ganglion. More substantial contracture and bone deformity at the shoulder is typical in postganglionic injuries. However, changes to the underlying muscle structure that drive these differences in presentation are unclear.
Methods: Seventeen Sprague-Dawley rats received preganglionic or postganglionic neurectomy on a single limb on postnatal days 3 and 4. Muscles crossing the shoulder were retrieved once the rats were sacrificed at 8 weeks after birth. External rotation range of motion, muscle mass, muscle length, muscle sarcomere length, and calculated optimal muscle length were measured bilaterally.
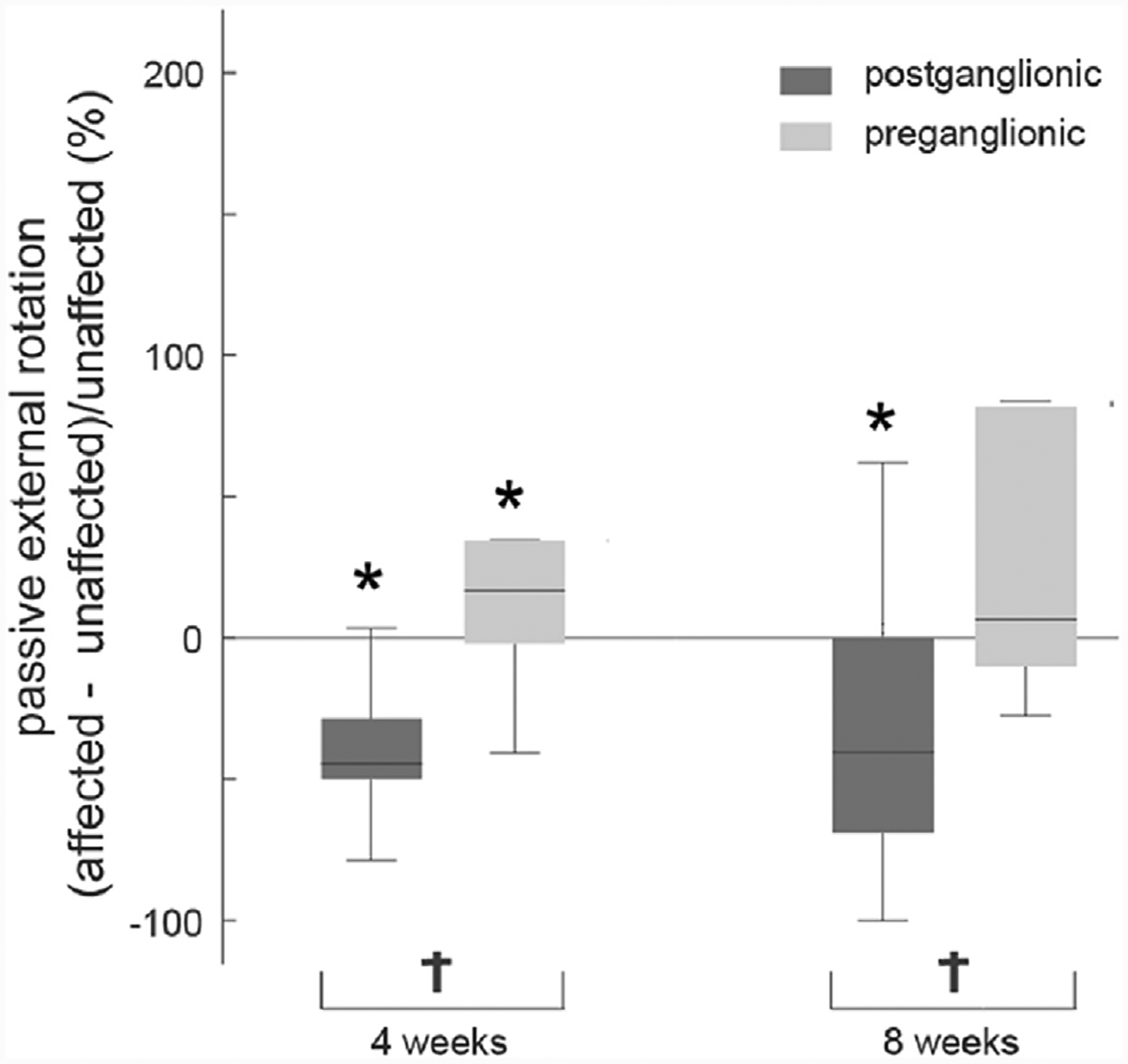
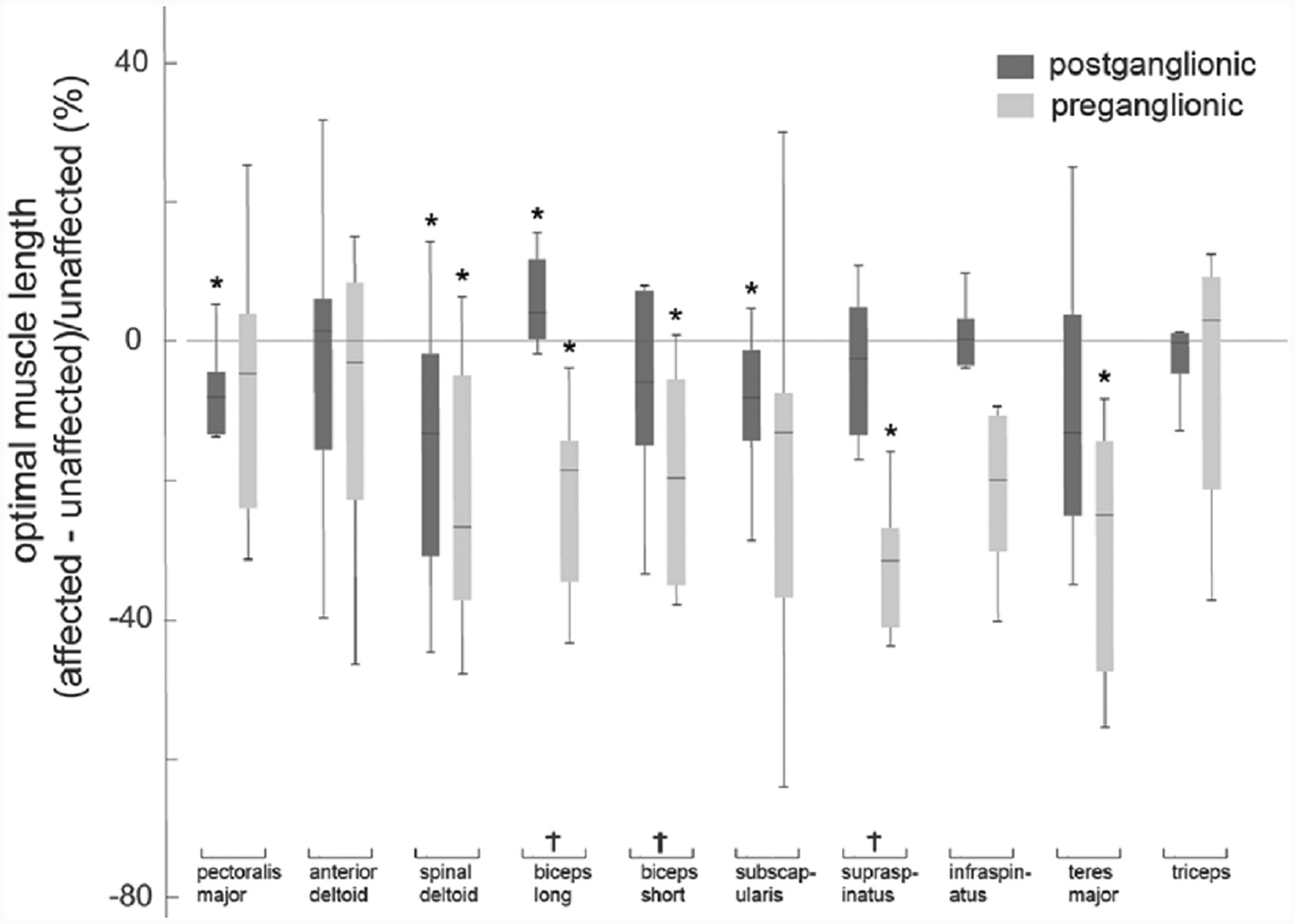
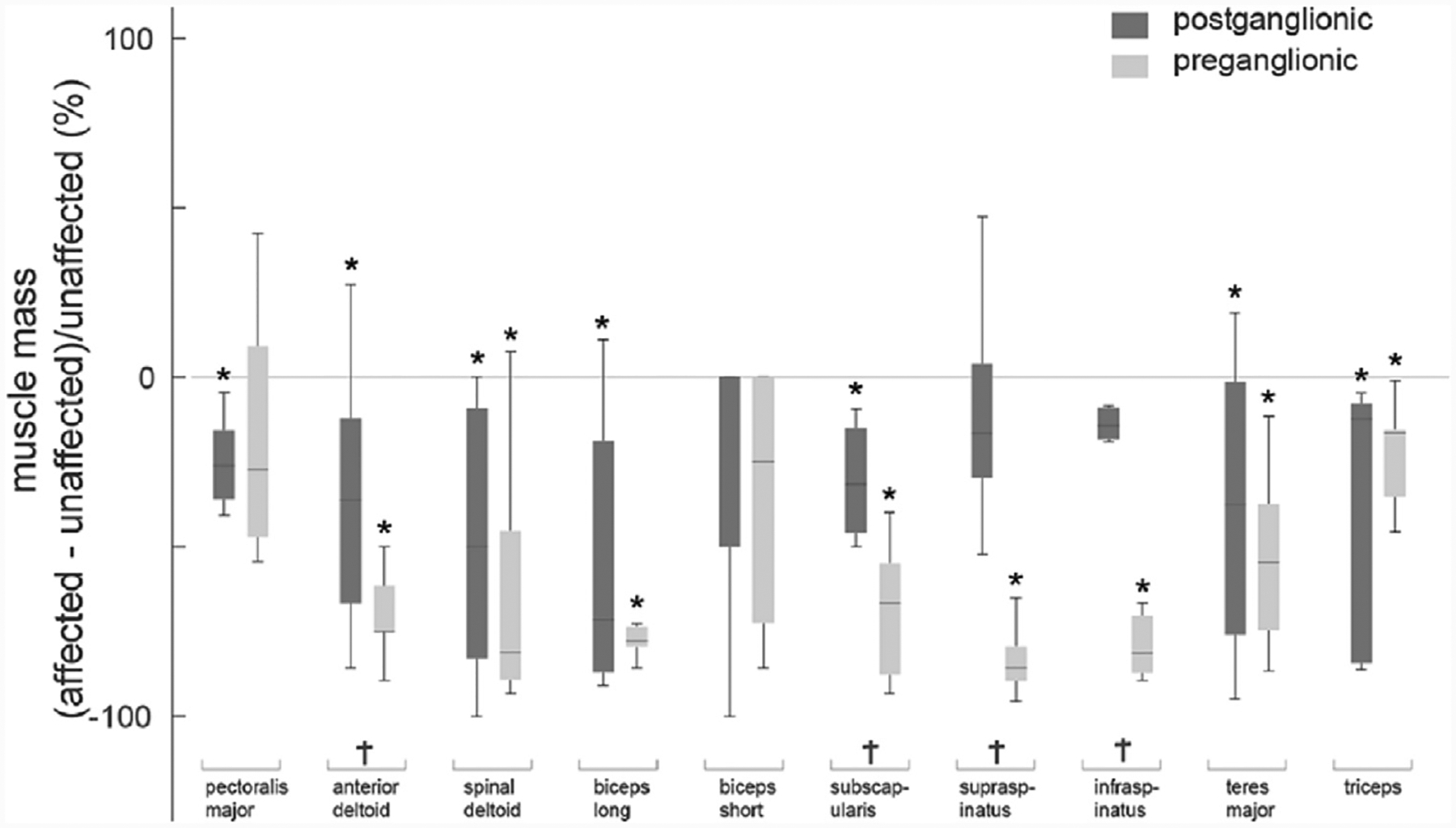
Results: Average shoulder range of motion in the postganglionic group was 61.8% and 56.2% more restricted at 4 and 8 weeks, respectively, compared with that in the preganglionic group, but affected muscles after preganglionic injury were altered more severely (compared with the unaffected limb) than after postganglionic injury. Optimal muscle length in preganglionic injury was shorter in the affected limb (compared with the unaffected limb: -18.2% ± 9.2%) and to a greater extent than in postganglionic injury (-5.1% ± 6.2%). Muscle mass in preganglionic injury was lower in the affected limb (relative to the unaffected limb: -57.2% ± 24.1%) and to a greater extent than in postganglionic injury (-28.1% ± 17.7%).
Conclusions: The findings suggest that the presence of contracture does not derive from restricted longitudinal muscle growth alone, but also depends on the extent of muscle mass loss occurring simultaneously after the injury.
Clinical relevance: This study expands our understanding of differences in muscle architecture and the role of muscle structure in contracture formation for preganglionic and postganglionic brachial plexus birth injury.
Keywords: Brachial plexus birth injury; contractures; muscle mass; range of motion; sarcomere length.
Copyright © 2021 American Society for Surgery of the Hand. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Foad SL, Mehlman CT, Ying J. The epidemiology of neonatal brachial plexus palsy in the united states. J Bone Joint Surg Am. 2008;90(6):1258–1264. - PubMed
-
- Lagerkvist A, Johansson U, Johansson A, Bager B, Uvebrant P. Obstetric brachial plexus palsy: a prospective, population-based study of incidence, recovery, and residual impairment at 18 months of age. Dev Med Child Neurol. 2010;52(6):529–534. - PubMed
-
- Pondaag W, Malessy MJ, Gert van Dijk J, Thomeer RT. Natural history of obstetric brachial plexus palsy: a systematic review. Dev Med Child Neurol. 2004;46(2):138–144. - PubMed
-
- Pearl ML. Shoulder problems in children with brachial plexus birth palsy: evaluation and management. J Am Acad Orthop Surg. 2009;17(4):242–254. - PubMed
-
- Bae D, Waters P, Zurakowski D. Correlation of pediatric outcomes data collection instrument with measures of active movement in children with brachial plexus. J Pediatr Orthop. 2008;28(5):584–592. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
