

Microsurgical ligation for incompletely coiled or recurrent intracranial aneurysms: a 17-year single-center experience
- PMID: 32922907
- PMCID: PMC7398258
- DOI: 10.1186/s41016-019-0153-z
Microsurgical ligation for incompletely coiled or recurrent intracranial aneurysms: a 17-year single-center experience
Abstract
Background: In this retrospective single-center study, we presented our experience in the microsurgical management of incompletely coiled or recurrent aneurysms after initial endovascular coiling.
Methods: During a 17-year period, 48 patients underwent microsurgical clipping of incompletely coiled or recurrent aneurysms after coiling (Gurian group B). The clinical data, surgical technique, and postoperative outcome were recorded and analyzed.
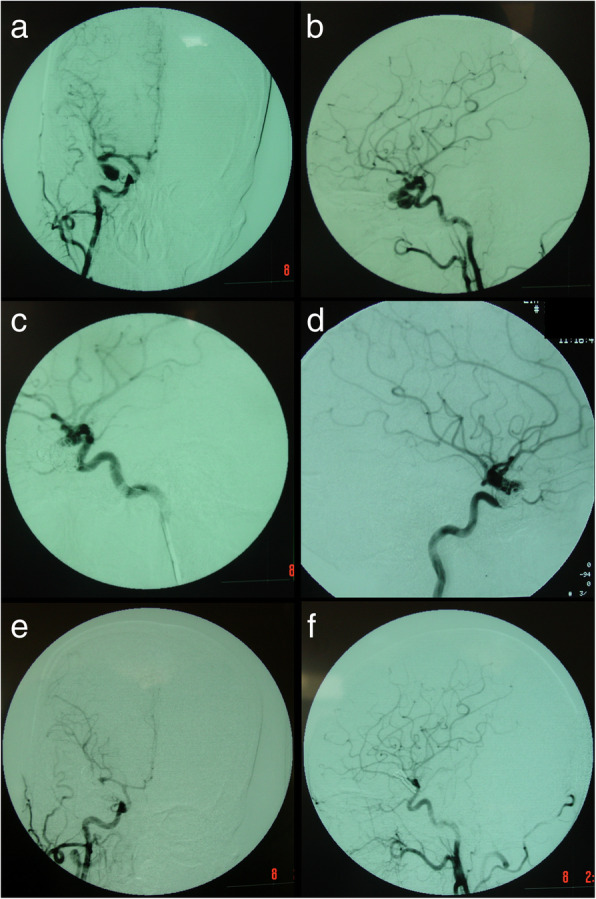
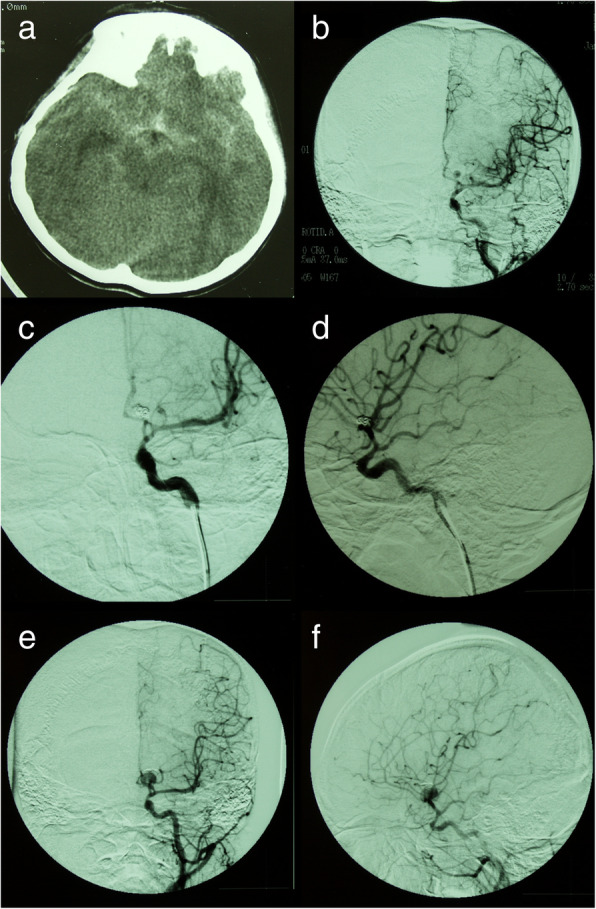
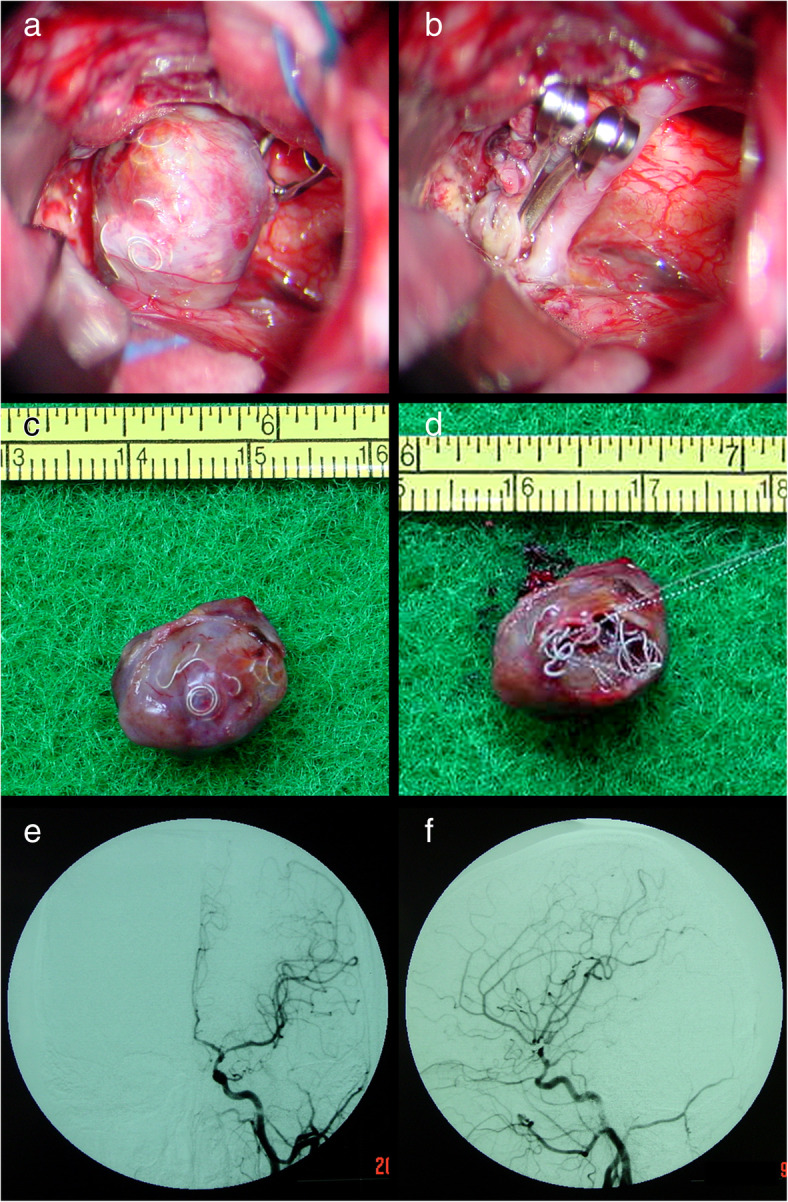
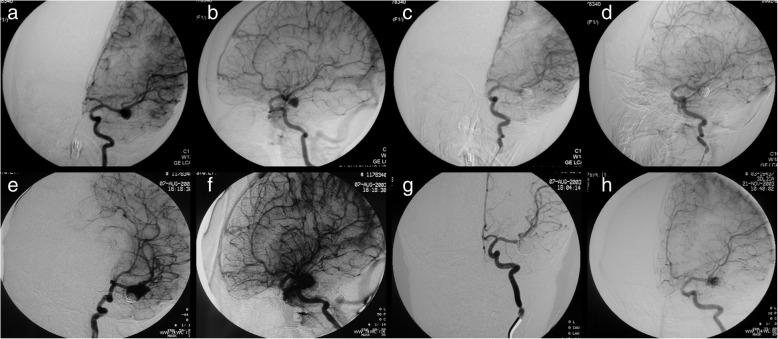
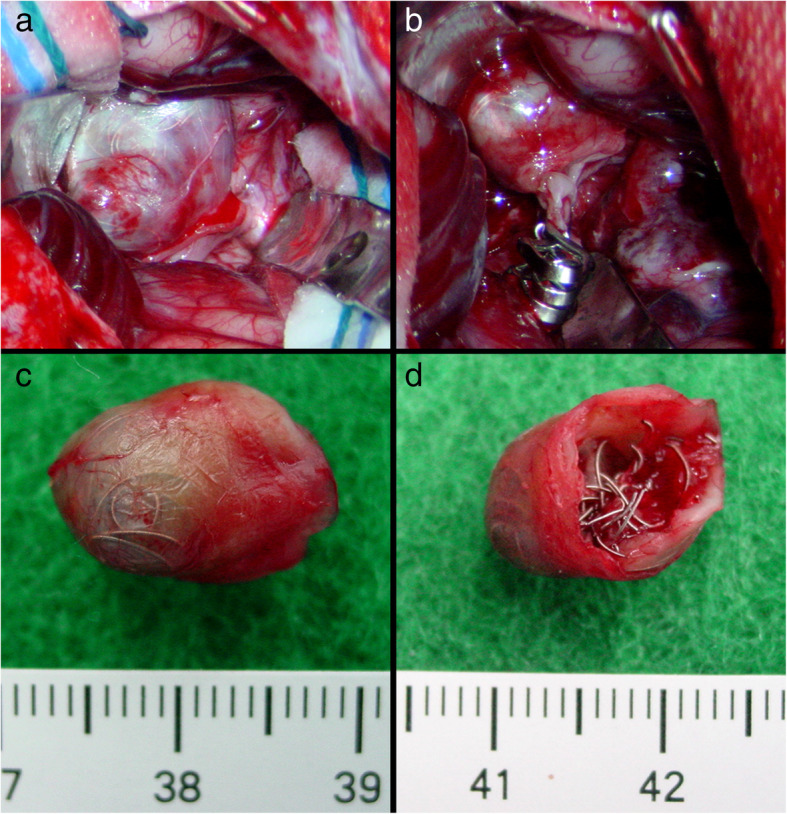
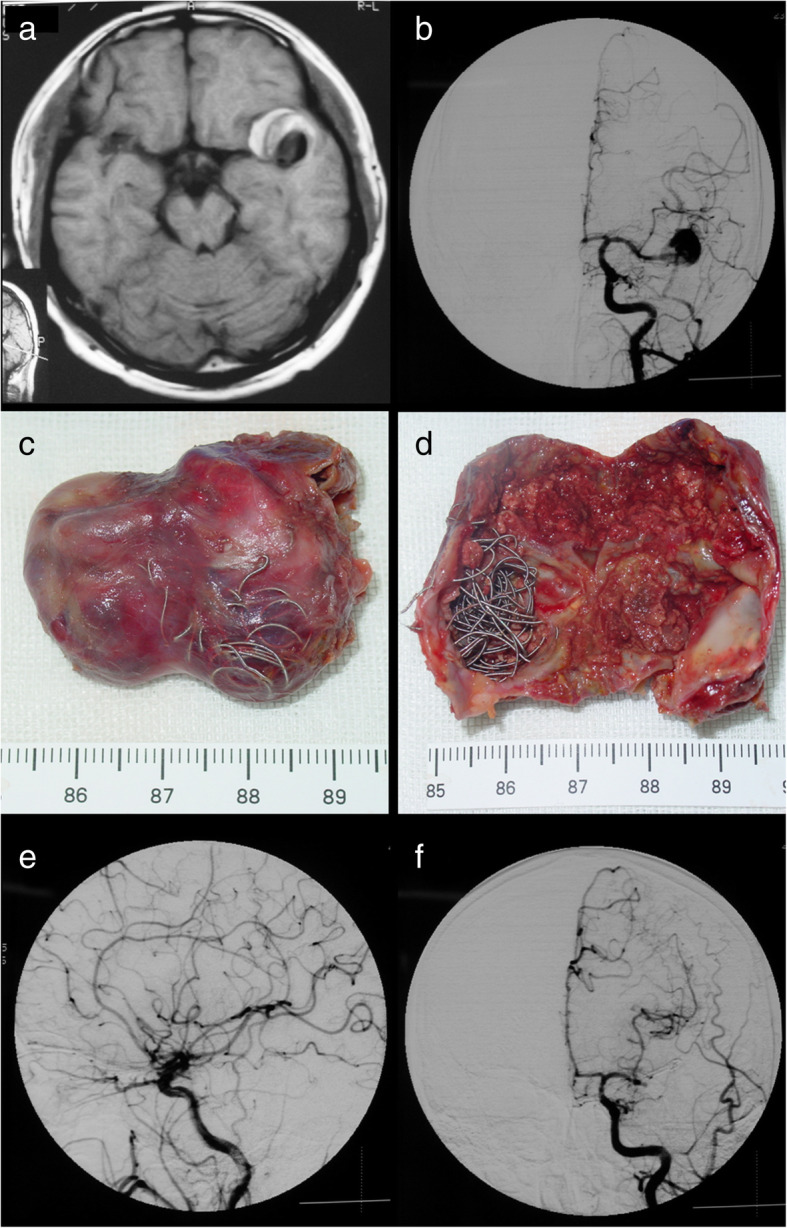
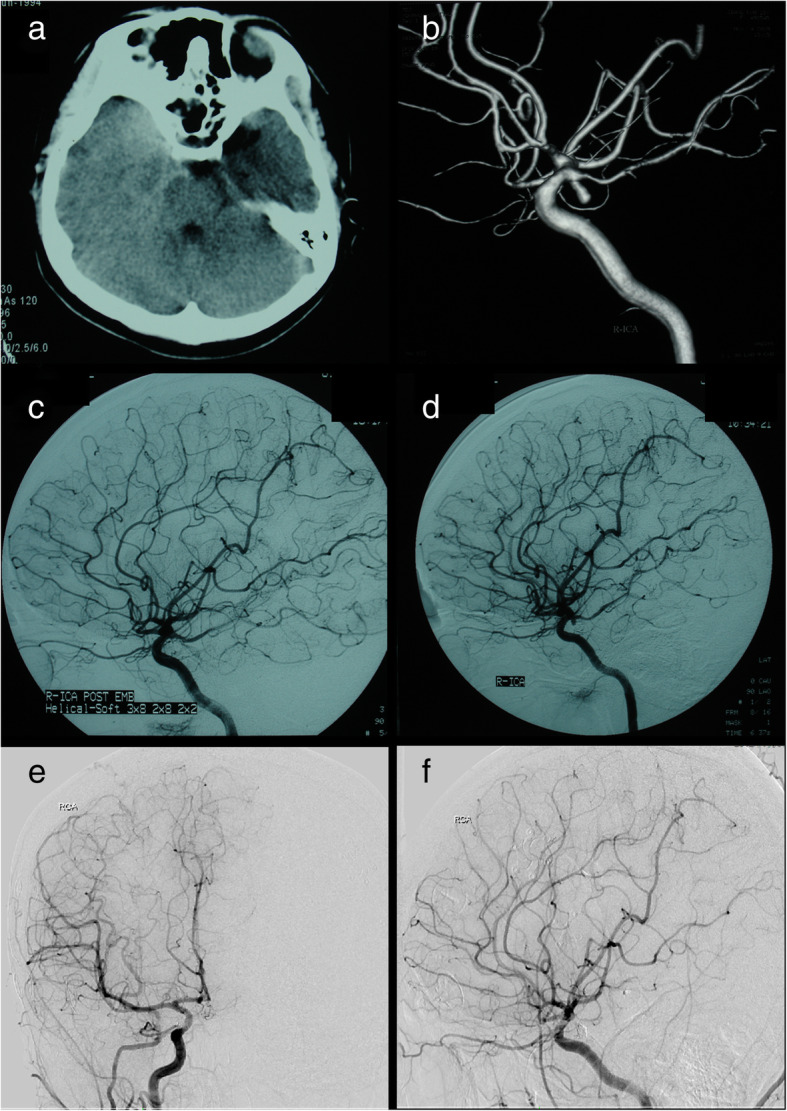
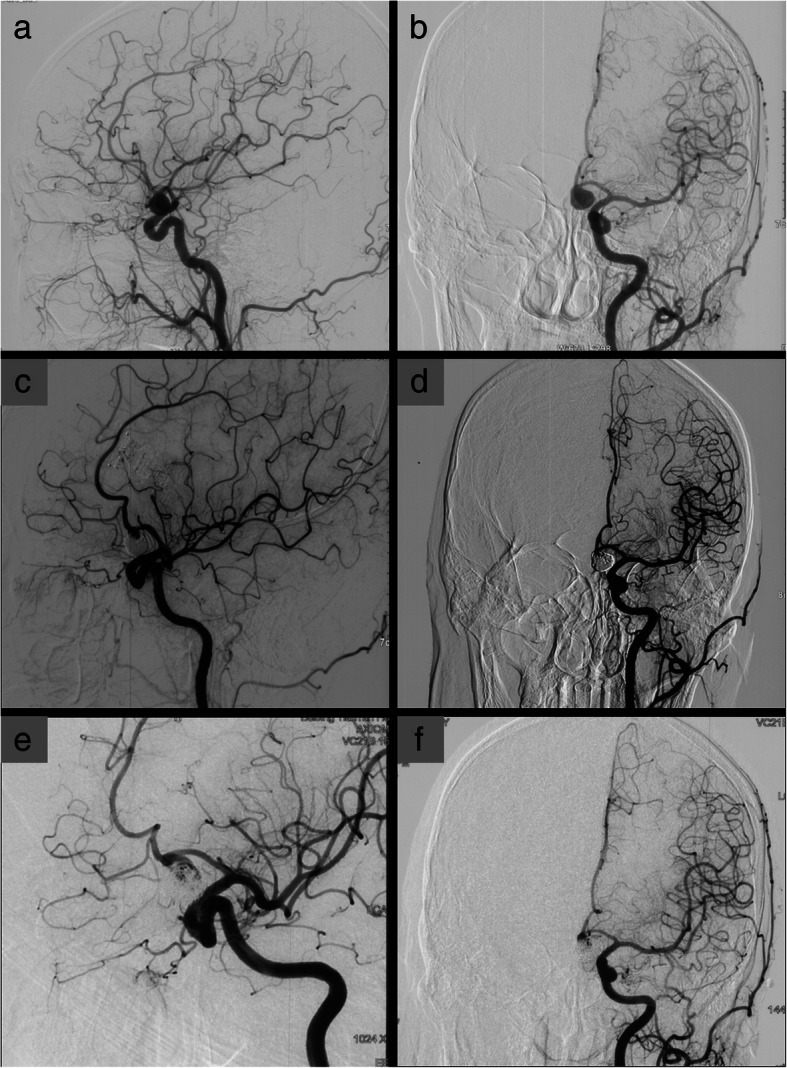
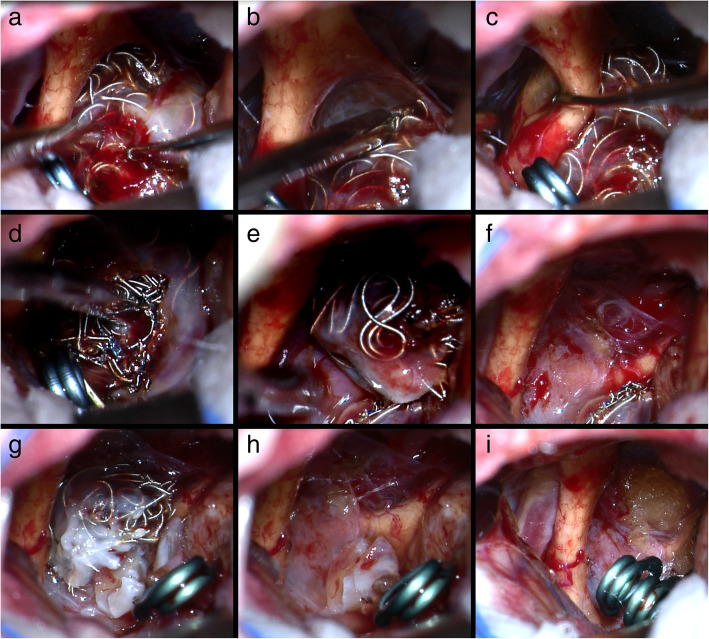
Results: Before coiling, 42 patients (87.5%) experienced aneurysm rupture. Most of the aneurysms (46/48, 96%) were located in the anterior circulation. After coiling, 6 patients had incompletely coiled aneurysms and 42 patients had recurrent aneurysms, with a mean time of 20.2 months from coiling to recurrence. Coil extrusion occurred in none of the incompletely coiled aneurysms and 71% (30/42) of the recurrent aneurysms. Clipping techniques are direct microsurgical clipping without coil removal in 16 patients, partial coil removal in 14 patients, and total coil removal in 18 patients. Postoperative and follow-up angiography revealed complete occlusion of the aneurysms in all patients. No patient died during postoperative follow-up period (mean, 78.9 months; range, 10-190 months). Good outcomes (GOS of 4 or 5) were achieved in 87.5% (42/48) of the patients at the final follow-up.
Conclusions: Microsurgical clipping is effective for incompletely coiled or recurrent aneurysms after initial coiling. For recurrent aneurysms that have coils in the neck, have no adequate neck for clipping, or cause mass effects on surrounding structures, partial or total removal of coiled mass can facilitate surgical clipping and lead to successful obliteration of the aneurysms.
Keywords: Coiled aneurysms; Endovascular coiling; Microsurgical clipping; Recurrent aneurysms.
© The Author(s) 2019.
Conflict of interest statement
Competing interestsAll authors certify that we have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements) or non-financial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript.
Figures
Similar articles
-
Microsurgical management of incompletely coiled and recurrent aneurysms: trends, techniques, and observations on coil extrusion.Neurosurgery. 2009 May;64(5 Suppl 2):301-15; discussion 315-7. doi: 10.1227/01.NEU.0000335178.15274.B4. Neurosurgery. 2009. PMID: 19404109
-
Microsurgical clipping for recurrent aneurysms after initial endovascular coil embolization.World Neurosurg. 2015 Feb;83(2):211-8. doi: 10.1016/j.wneu.2014.08.013. Epub 2014 Aug 10. World Neurosurg. 2015. PMID: 25118057
-
Microsurgical clipping of previously coiled intracranial aneurysms.Clin Neurol Neurosurg. 2013 Aug;115(8):1343-9. doi: 10.1016/j.clineuro.2012.12.030. Epub 2013 Jan 24. Clin Neurol Neurosurg. 2013. PMID: 23352715
-
Microsurgical Treatment of Previously Coiled Giant Aneurysms: Experience with 6 Cases and Literature Review.World Neurosurg. 2023 Mar;171:e336-e348. doi: 10.1016/j.wneu.2022.12.016. Epub 2022 Dec 10. World Neurosurg. 2023. PMID: 36513298 Review.
-
MICROSURGICAL MANAGEMENT OF RECURRENT INTRACRANIAL ANEURYSMS FOLLOWING ENDOVASCULAR TREATMENT: A SINGLE INSTITUTION ILLUSTRATIVE CASE SERIES AND LITERATURE REVIEW.Acta Clin Croat. 2021 Dec;60(4):695-702. doi: 10.20471/acc.2021.60.04.17. Acta Clin Croat. 2021. PMID: 35734492 Free PMC article. Review.
Cited by
-
Woven endo bridge device for recurrent intracranial aneurysms: A systematic review and meta-analysis.Neuroradiol J. 2024 Dec;37(6):688-698. doi: 10.1177/19714009241247457. Epub 2024 Apr 13. Neuroradiol J. 2024. PMID: 38613671
-
Disturbed flow's impact on cellular changes indicative of vascular aneurysm initiation, expansion, and rupture: A pathological and methodological review.J Cell Physiol. 2022 Jan;237(1):278-300. doi: 10.1002/jcp.30569. Epub 2021 Sep 6. J Cell Physiol. 2022. PMID: 34486114 Free PMC article. Review.
-
Microsurgical management of previously embolized intracranial aneurysms: A single center experience and literature review.J Cerebrovasc Endovasc Neurosurg. 2025 Mar;27(1):1-18. doi: 10.7461/jcen.2024.E2024.05.004. Epub 2024 Dec 17. J Cerebrovasc Endovasc Neurosurg. 2025. PMID: 39681331 Free PMC article.
-
Surgical Clipping of Previously Coiled Recurrent Intracranial Aneurysms: A Single-Center Experience.Front Neurol. 2021 Sep 21;12:680375. doi: 10.3389/fneur.2021.680375. eCollection 2021. Front Neurol. 2021. PMID: 34621232 Free PMC article.
References
-
- Arnaout OM, El Ahmadieh TY, Zammar SG, El Tecle NE, Hamade YJ, Aoun RJ, Aoun SG, Rahme RJ, Eddleman CS, Barrow DL, Batjer HH, Bendok BR. Microsurgical treatment of previously coiled intracranial aneurysms: systematic review of the literature. World Neurosurg. 2015;84:246–253. doi: 10.1016/j.wneu.2015.02.027. - DOI - PubMed
-
- Campi A, Ramzi N, Molyneux AJ, Summers PE, Kerr RS, Sneade M, Yarnold JA, Rischmiller J, Byrne JV. Retreatment of ruptured cerebral aneurysms in patients randomized by coiling or clipping in the International Subarachnoid Aneurysm Trial (ISAT) Stroke. 2007;38:1538–1544. doi: 10.1161/STROKEAHA.106.466987. - DOI - PubMed
LinkOut - more resources
Full Text Sources