

Machine Learning-Based Radiomics Nomogram Using Magnetic Resonance Images for Prediction of Neoadjuvant Chemotherapy Efficacy in Breast Cancer Patients
- PMID: 32923392
- PMCID: PMC7456979
- DOI: 10.3389/fonc.2020.01410
Machine Learning-Based Radiomics Nomogram Using Magnetic Resonance Images for Prediction of Neoadjuvant Chemotherapy Efficacy in Breast Cancer Patients
Abstract
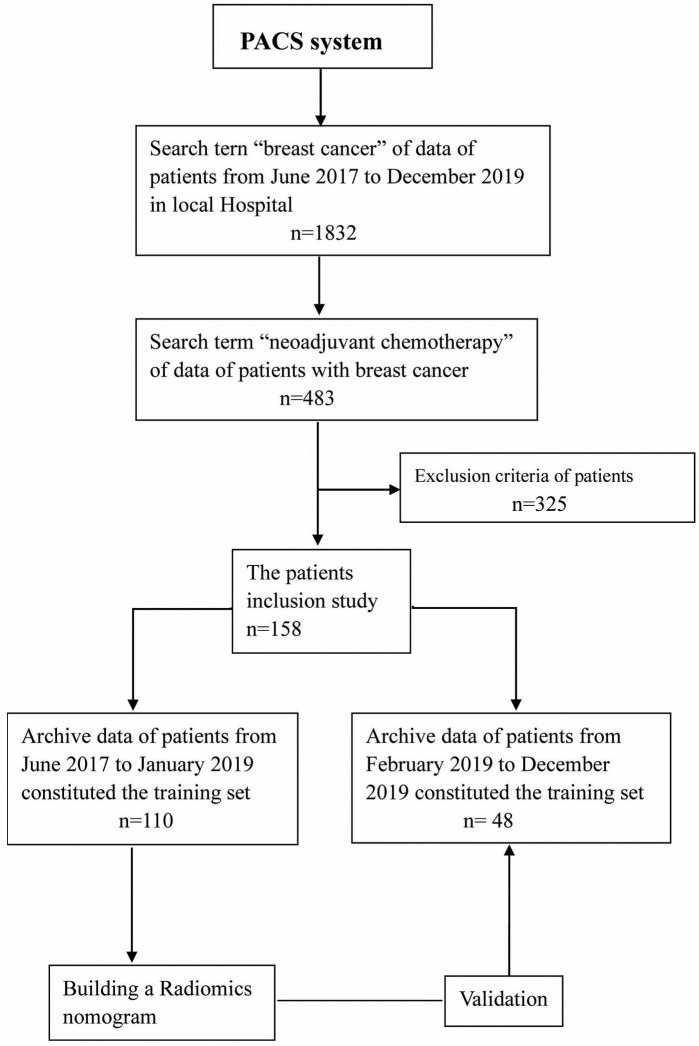
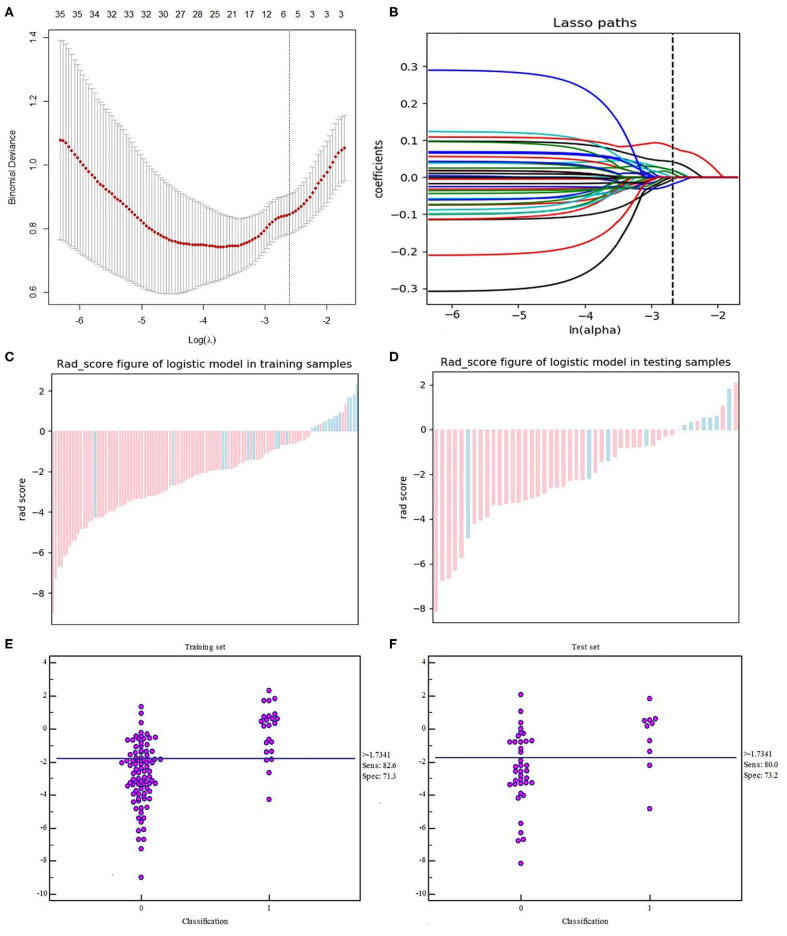
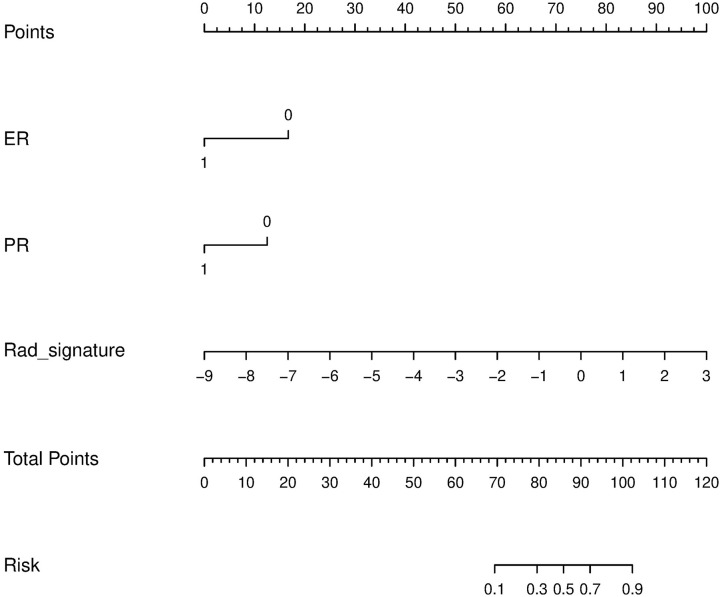
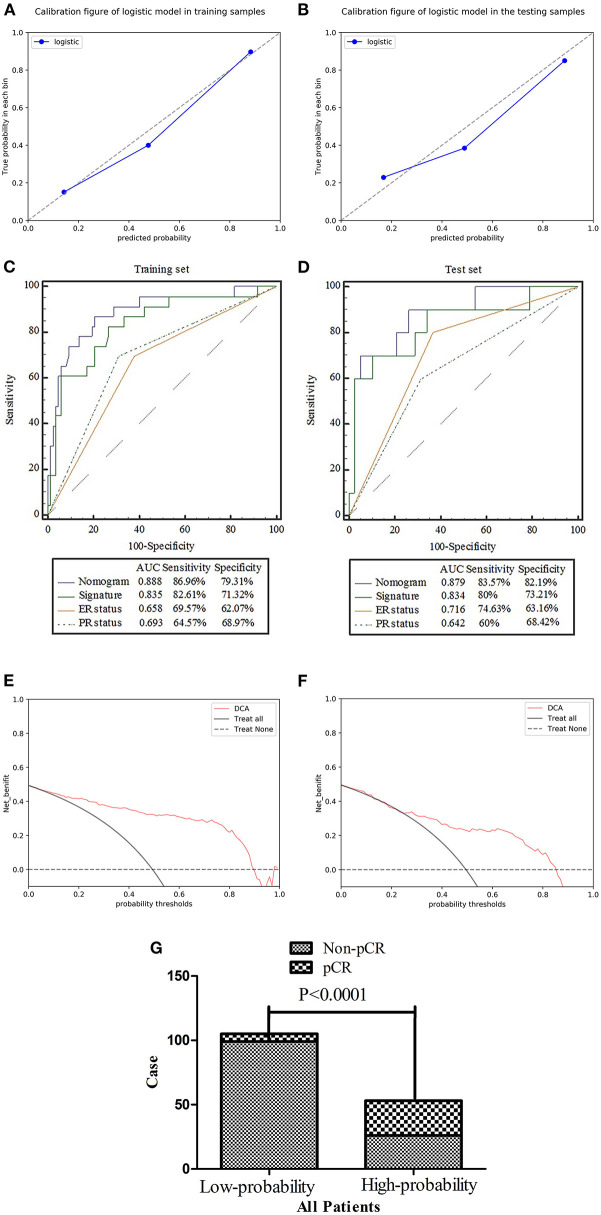
Purpose: The construction and validation of a radiomics nomogram based on machine learning using magnetic resonance image (MRI) for predicting the efficacy of neoadjuvant chemotherapy (NACT) in patients with breast cancer (BCa). Methods: This retrospective investigation consisted of 158 patients who were diagnosed with BCa and underwent MRI before NACT, of which 33 patients experienced pathological complete response (pCR) by the postoperative pathological examination. The patients with BCa were divided into the training set (n = 110) and test set (n = 48) randomly. The features were selected by the maximum relevance minimum redundancy (mRMR) and absolute shrinkage and selection operator (LASSO) algorithm in the training set. In return, the radiomics signature was established using machine learning. The predictive score of each patient was calculated using the radiomics signature formula. Finally, the predictive scores and clinical factors were used to perform the multivariate logistic regression and construct the nomogram. Receiver operating characteristics (ROC) analyses were used to assess and validate the diagnostic accuracy of the nomogram in the test set. Lastly, the usefulness of the nomogram was confirmed via decision curve analysis (DCA). Results: The radiomics signature was well-discriminated in the training set [AUC 0.835, specificity 71.32%, and sensitivity 82.61%], and test set (AUC 0.834, specificity 73.21%, and sensitivity 80%). Containing the radiomics signature and hormone status, the radiomics nomogram showed good calibration and discrimination in the training set [AUC 0.888, specificity 79.31%, and sensitivity 86.96%] and test set (AUC 0.879, specificity 82.19%, and sensitivity 83.57%). The decision curve indicated the clinical usefulness of our nomogram. Conclusion: Our radiomics nomogram showed good discrimination in patients with BCa who experience pCR after NACT. The model may aid physicians in predicting how specific patients may respond to BCa treatments in the future.
Keywords: breast cancer; machine learning; neoadjuvant chemotherapy; nomogram; pathological complete response; radiomics.
Copyright © 2020 Chen, Shu, Li, Chen, Tang, Mo, Shao and Shao.
Figures

References
-
- Early Breast Cancer Trialists' Collaborative Group (EBCTCG) . Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. (2018) 19:27–39. 10.1016/S1470-2045(17)30777-5 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources