

Modeling of Xerostomia After Radiotherapy for Head and Neck Cancer: A Registry Study
- PMID: 32923404
- PMCID: PMC7456883
- DOI: 10.3389/fonc.2020.01647
Modeling of Xerostomia After Radiotherapy for Head and Neck Cancer: A Registry Study
Abstract
Aim: Data from a local quality registry are used to model the risk of late xerostomia after radiotherapy for head and neck cancer (HNC), based on dosimetric- and clinical variables. Strengths and weaknesses of using quality registry data are explored.
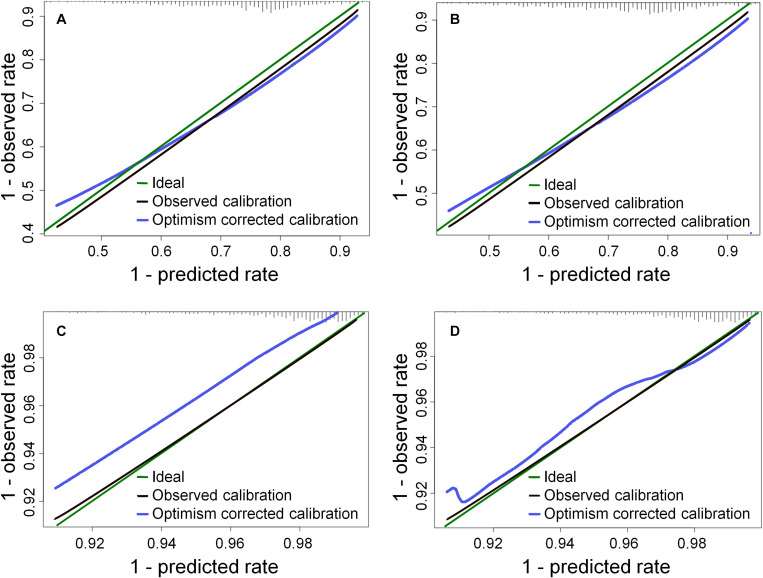
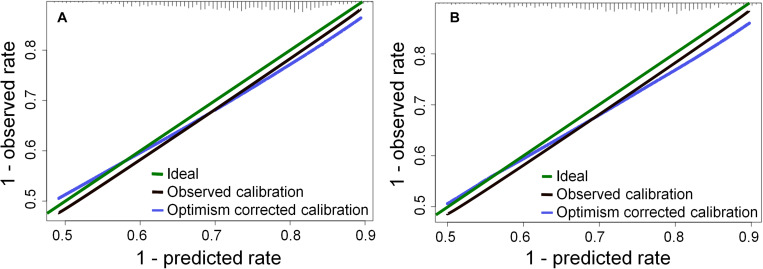
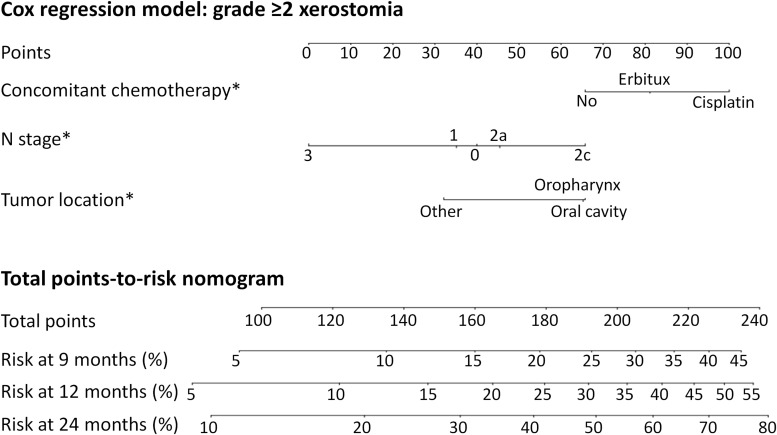
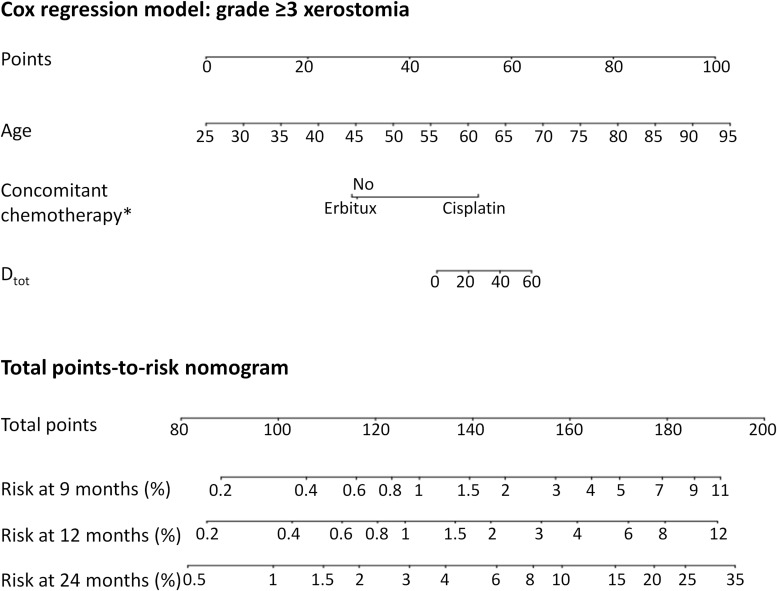
Methods: HNC patients treated with radiotherapy at the Karolinska University hospital are entered into a quality registry at routine follow up, recording morbidity according to a modified RTOG/LENT-SOMA scale. Other recorded parameters are performance status, age, gender, tumor location, tumor stage, smoking status, chemotherapy and radiotherapy data, including prescribed dose and organ-at-risk (OAR) dose. Most patients are entered at several time points, but at variable times after treatment. Xerostomia was modeled based on follow-up data from January 2014 to October 2018, resulting in 753 patients. Two endpoints were considered: maximum grade ≥2 (XERG≥2) or grade ≥3 (XERG≥3) late xerostomia. Univariate Cox regression was used to select variables for two multivariate models for each endpoint, one based on the mean dose to the total parotid volume (Dtot) and one based on the mean dose to the contralateral parotid (Dcontra). Cox regression allows the estimation of the risk of xerostomia at different time points; models were presented visually as nomograms estimating the risk at 9, 12, and 24 months respectively.
Results: The toxicity rates were 366/753 (49%) for XERG≥2 and 40/753 (5.3%) for XERG≥3. The multivariate models included several variables for XERG≥2, and dose, concomitant chemotherapy and age were included for XERG≥3. Induction chemotherapy and an increased number of fractions per week were associated with a lower risk of XERG≥2. However, since the causality of these relationships have limited support from previous studies, alternative models without these variables were also presented. The models based on the mean dose to the total parotid volume and the contralateral parotid alone were very similar.
Conclusion: Late xerostomia after radiotherapy can be modeled with reasonable predictive power based on registry data; models are presented for different endpoints highly relevant in clinical practice. However, the risk of modeling indirect relationships, given the unavoidably heterogeneous registry data, needs to be carefully considered in the interpretation of the results.
Keywords: cox regression; head and neck cancer; nomogram; registry analysis; xerostomia.
Copyright © 2020 Onjukka, Mercke, Björgvinsson, Embring, Berglund, Alexandersson von Döbeln, Friesland, Gagliardi, Lenneby Helleday, Sjödin and Lax.
Figures
Similar articles
-
NTCP models for patient-rated xerostomia and sticky saliva after treatment with intensity modulated radiotherapy for head and neck cancer: the role of dosimetric and clinical factors.Radiother Oncol. 2012 Oct;105(1):101-6. doi: 10.1016/j.radonc.2012.03.004. Epub 2012 Apr 18. Radiother Oncol. 2012. PMID: 22516776
-
Can dose reduction to one parotid gland prevent xerostomia?--A feasibility study for locally advanced head and neck cancer patients treated with intensity-modulated radiotherapy.Clin Oncol (R Coll Radiol). 2006 Aug;18(6):497-504. doi: 10.1016/j.clon.2006.04.014. Clin Oncol (R Coll Radiol). 2006. PMID: 16909975 Clinical Trial.
-
Development of NTCP models for head and neck cancer patients treated with three-dimensional conformal radiotherapy for xerostomia and sticky saliva: the role of dosimetric and clinical factors.Radiother Oncol. 2012 Oct;105(1):86-93. doi: 10.1016/j.radonc.2011.05.010. Epub 2011 May 31. Radiother Oncol. 2012. PMID: 21632133
-
Risk model and nomogram for dysphagia and xerostomia prediction in head and neck cancer patients treated by radiotherapy and/or chemotherapy.Dysphagia. 2013 Sep;28(3):388-94. doi: 10.1007/s00455-012-9445-6. Epub 2013 Jan 26. Dysphagia. 2013. PMID: 23355106
-
Early prediction of radiotherapy-induced parotid shrinkage and toxicity based on CT radiomics and fuzzy classification.Artif Intell Med. 2017 Sep;81:41-53. doi: 10.1016/j.artmed.2017.03.004. Epub 2017 Mar 18. Artif Intell Med. 2017. PMID: 28325604
Cited by
-
The Role of Patient- and Treatment-Related Factors and Early Functional Imaging in Late Radiation-Induced Xerostomia in Oropharyngeal Cancer Patients.Cancers (Basel). 2021 Dec 15;13(24):6296. doi: 10.3390/cancers13246296. Cancers (Basel). 2021. PMID: 34944916 Free PMC article.
-
A Risk Prediction Model by LASSO for Radiation-Induced Xerostomia in Patients With Nasopharyngeal Carcinoma Treated With Comprehensive Salivary Gland-Sparing Helical Tomotherapy Technique.Front Oncol. 2021 Feb 26;11:633556. doi: 10.3389/fonc.2021.633556. eCollection 2021. Front Oncol. 2021. PMID: 33718219 Free PMC article.
-
Clinical Introduction of Stem Cell Sparing Radiotherapy to Reduce the Risk of Xerostomia in Patients with Head and Neck Cancer.Cancers (Basel). 2024 Dec 23;16(24):4283. doi: 10.3390/cancers16244283. Cancers (Basel). 2024. PMID: 39766181 Free PMC article.
-
Modelling Radiation-Induced Salivary Dysfunction during IMRT and Chemotherapy for Nasopharyngeal Cancer Patients.Cancers (Basel). 2021 Aug 6;13(16):3983. doi: 10.3390/cancers13163983. Cancers (Basel). 2021. PMID: 34439136 Free PMC article.
-
Validated prediction of xerostomia in a real-world population: a step toward model-guided radiotherapy.Acta Oncol. 2025 Aug 18;64:1087-1094. doi: 10.2340/1651-226X.2025.43462. Acta Oncol. 2025. PMID: 40823804 Free PMC article.
References
-
- Langendijk JA, Doornaert P, Verdonck-de Leeuw IM, Leemans CR, Aaronson NK, Slotman BJ. Impact of late treatment-related toxicity on quality of life among patients with head and neck cancer treated with radiotherapy. J Clin Oncol. (2008) 26:3770–6. - PubMed
-
- Dirix P, Nuyts S, Van den Bogaert W. Radiation-induced xerostomia in patients with head and neck cancer: a literature review. Cancer. (2006) 107:2525–34. - PubMed
LinkOut - more resources
Full Text Sources