

Impact of a Cancer Gene Variant Reclassification Program Over a 20-Year Period
- PMID: 32923914
- PMCID: PMC7469614
- DOI: 10.1200/PO.20.00020
Impact of a Cancer Gene Variant Reclassification Program Over a 20-Year Period
Abstract
Purpose: Hereditary cancer genetic testing can inform personalized medical management for individuals at increased cancer risk. However, many variants in cancer predisposition genes are individually rare, and traditional tools may be insufficient to evaluate pathogenicity. This analysis presents data on variant classification and reclassification over a 20-year period.
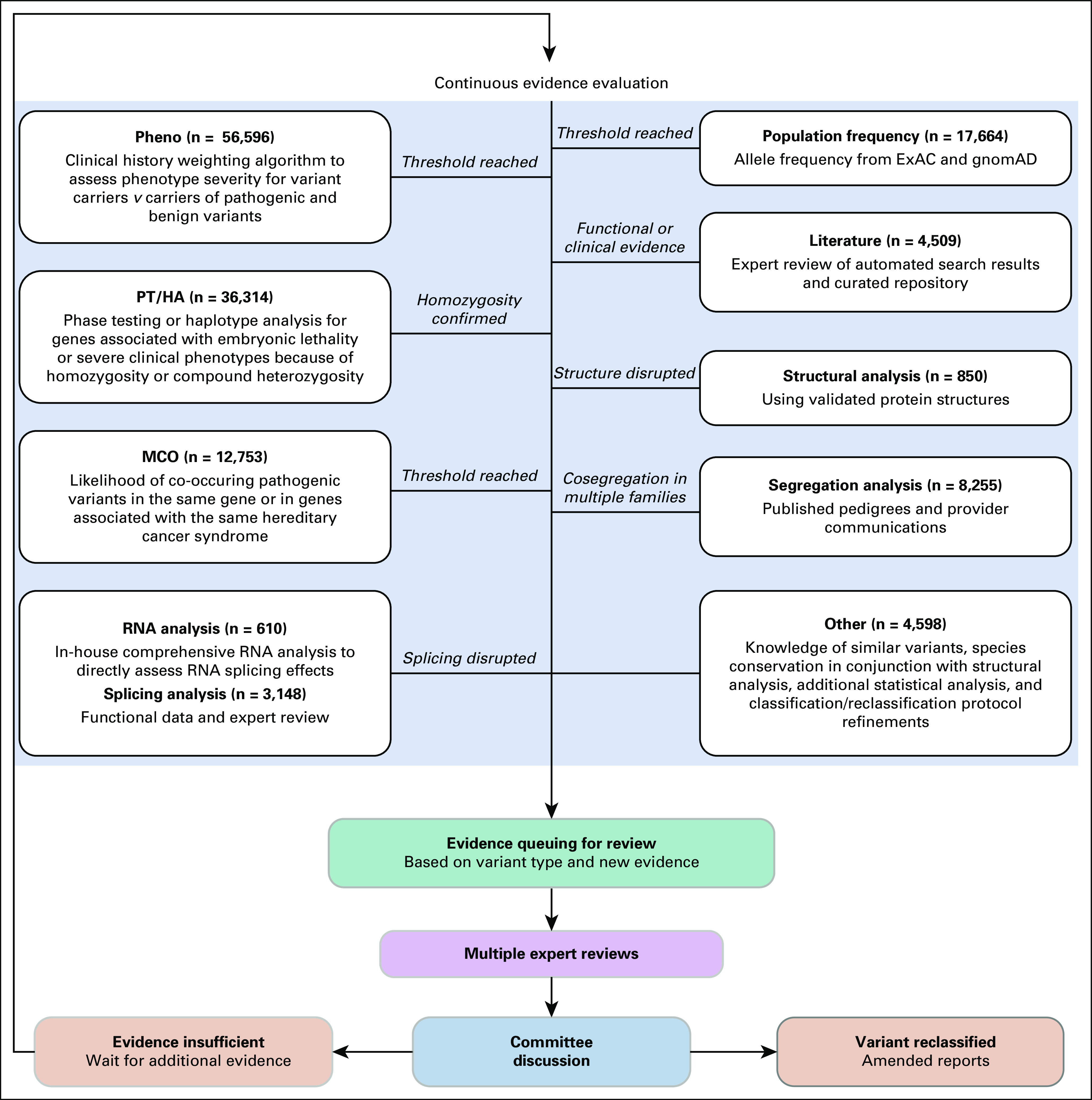
Patients and methods: This is a retrospective analysis of > 1.9 million individuals who received hereditary cancer genetic testing from a single clinical laboratory (March 1997 to December 2017). Variant classification included review of evidence from traditional tools (eg, population frequency databases, literature) and laboratory-developed tools (eg, novel statistical methods, in-house RNA analysis) by a multidisciplinary expert committee. Variants may have been reclassified more than once and with more than one line of evidence.
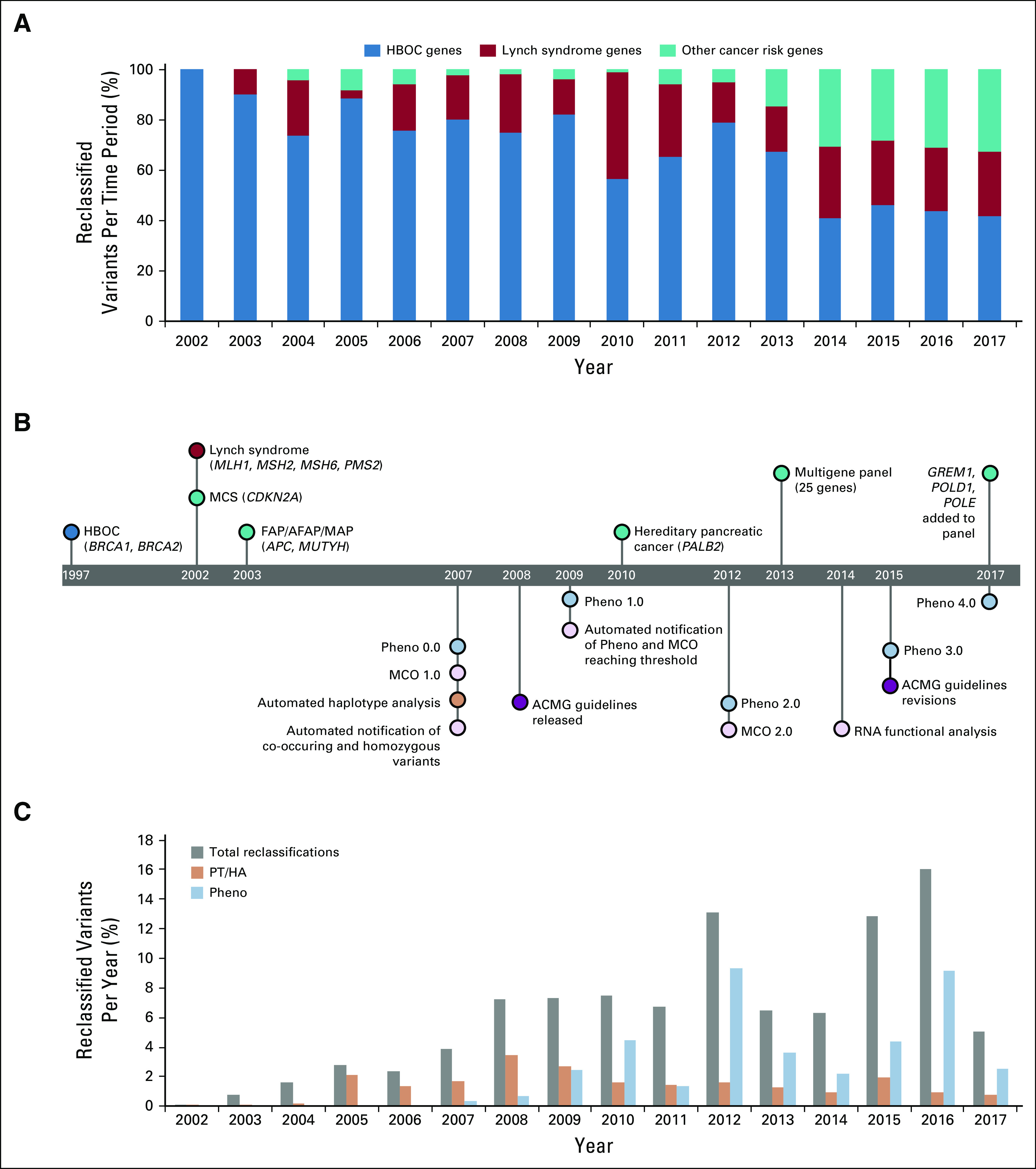
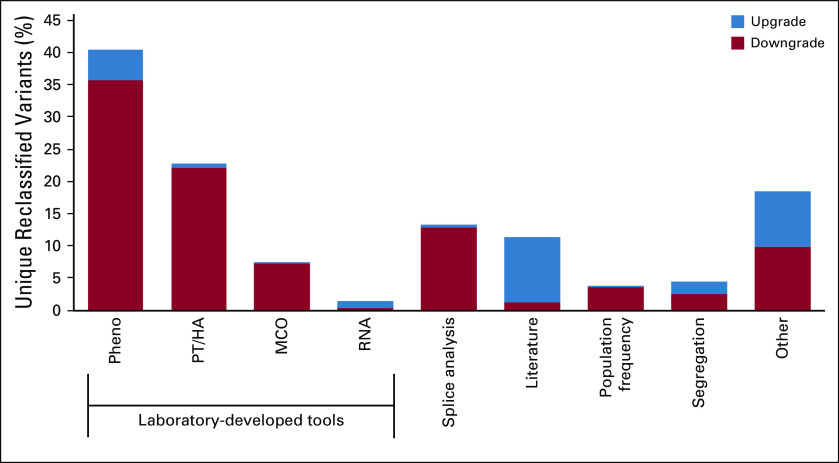
Results: In this time period, 62,842 unique variants were observed across 25 cancer predisposition genes, and 2,976 variants were reclassified. Overall, 82.1% of reclassification events were downgrades (eg, variant of uncertain significance [VUS] to benign), and 17.9% were upgrades (eg, VUS to pathogenic). Among reclassified variants, 82.8% were initially classified as VUS, and 47.5% were identified in ≤ 20 individuals (allele frequency ≤ 0.001%). Laboratory-developed tools were used in 72.3% of variant reclassification events, which affected > 600,000 individuals. More than 1.3 million patients were identified as carrying a variant that was reclassified within this 20-year time period.
Conclusion: The variant classification program used by the laboratory evaluated here enabled the reclassification of variants that were individually rare. Laboratory-developed tools were a key component of this program and were used in the majority of reclassifications. This demonstrates the importance of using robust and novel tools to reclassify rare variants to appropriately inform personalized medical management.
© 2020 by American Society of Clinical Oncology.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/po/author-center. Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments). Lisa EsterlingEmployment: Myriad Genetics Stock and Other Ownership Interests: Myriad GeneticsKrystal BrownEmployment: Myriad Genetics Stock and Other Ownership Interests: Myriad GeneticsBrian MorrisEmployment: Myriad Genetics Stock and Other Ownership Interests: Myriad GeneticsElisha HughesEmployment: Myriad Genetics Stock and Other Ownership Interests: Myriad GeneticsDmitry PrussEmployment: Myriad Genetics Stock and Other Ownership Interests: Myriad GeneticsSusan ManleyEmployment: Myriad Genetics Stock and Other Ownership Interests: Myriad GeneticsKarla R. BowlesEmployment: Myriad Genetic Laboratories Leadership: Myriad Genetic Laboratories Stock and Other Ownership Interests: Myriad GeneticsTheodora S. RossEmployment: Merck & Co. No other potential conflicts of interest were reported.
Figures
References
-
- Daly MB, Pilarski R, Berry M, et al. NCCN Guidelines Version 1.2020 Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic. Plymouth Meeting, PA, National Comprehensive Cancer Network, 2019. - PubMed
-
- Rosenthal ET, Bowles KR, Pruss D, et al. Exceptions to the rule: Case studies in the prediction of pathogenicity for genetic variants in hereditary cancer genes. Clin Genet. 2015;88:533–541. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
