

Penetrance of Colorectal Cancer Among Mismatch Repair Gene Mutation Carriers: A Meta-Analysis
- PMID: 32923933
- PMCID: PMC7476651
- DOI: 10.1093/jncics/pkaa027
Penetrance of Colorectal Cancer Among Mismatch Repair Gene Mutation Carriers: A Meta-Analysis
Abstract
Background: Lynch syndrome, the most common colorectal cancer (CRC) syndrome, is caused by germline mismatch repair (MMR) genes. Precise estimates of age-specific risks are crucial for sound counseling of individuals managing a genetic predisposition to cancer, but published risk estimates vary. The objective of this work is to provide gene-, sex-, and age-specific risk estimates of CRC for MMR mutation carriers that comprehensively reflect the best available data.
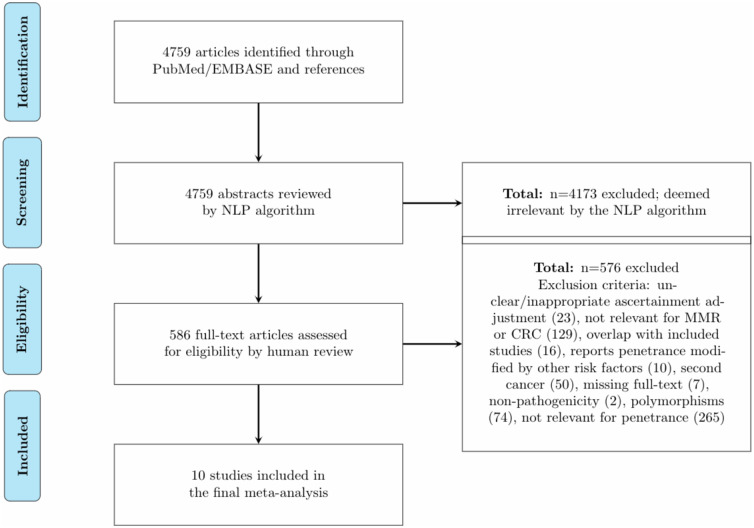
Methods: We conducted a meta-analysis to combine risk information from multiple studies on Lynch syndrome-associated CRC. We used a likelihood-based approach to integrate reported measures of CRC risk and deconvolved aggregated information to estimate gene- and sex-specific risk.
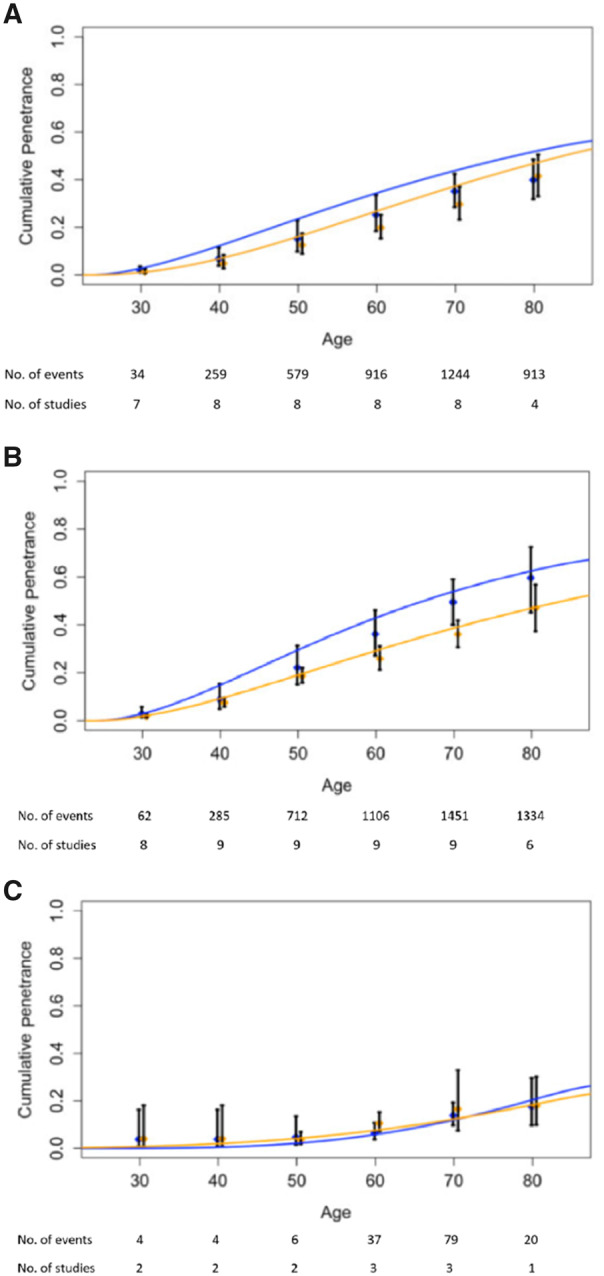
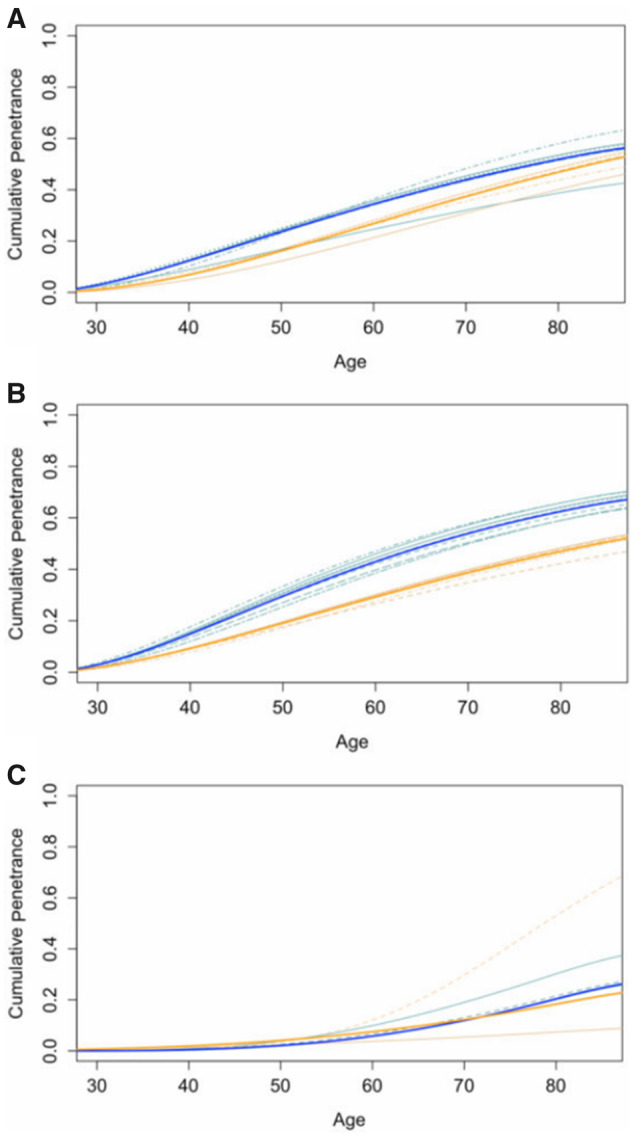
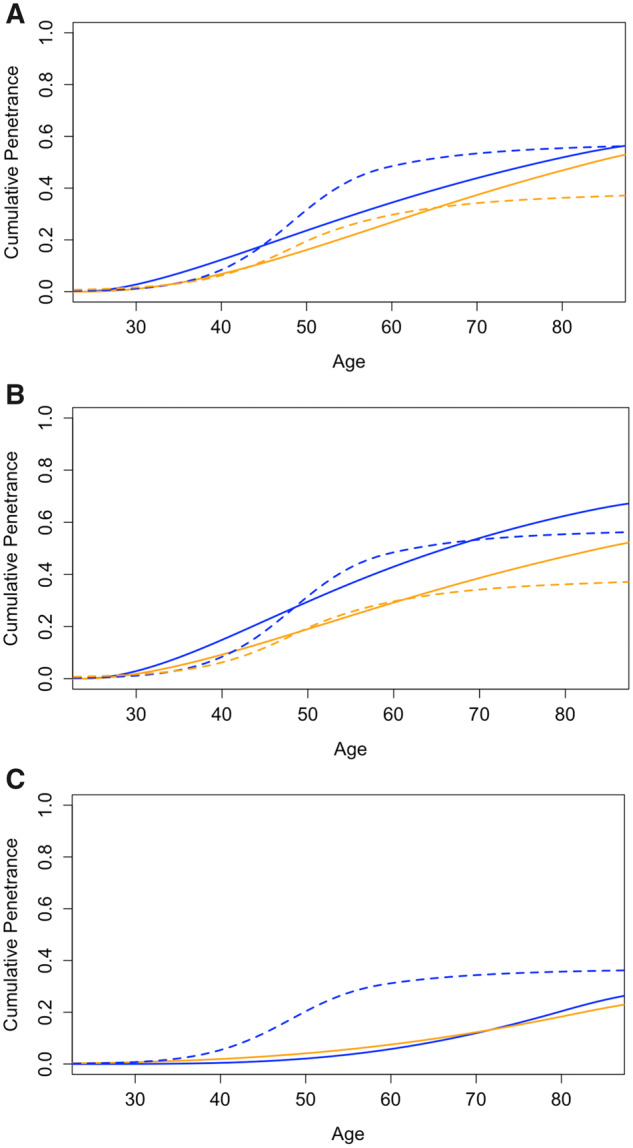
Results: Our comprehensive search identified 10 studies (8 on MLH1, 9 on MSH2, and 3 on MSH6). We estimated the cumulative risk of CRC by age and sex in heterozygous mutation carriers. At age 70 years, for male and female carriers, respectively, risks for MLH1 were 43.9% (95% confidence interval [CI] = 39.6% to 46.6%) and 37.3% (95% CI = 32.2% to 40.2%), for MSH2 were 53.9% (95% CI = 49.0% to 56.3%) and 38.6% (95% CI = 34.1% to 42.0%), and for MSH6 were 12.0% (95% CI = 2.4% to 24.6%) and 12.3% (95% CI = 3.5% to 23.2%).
Conclusions: Our results provide up-to-date and comprehensive age-specific CRC risk estimates for counseling and risk prediction tools. These will have a direct clinical impact by improving prevention and management strategies for both individuals who are MMR mutation carriers and those considering testing.
© The Author(s) 2020. Published by Oxford University Press.
Figures

Comment in
-
Refining Risk Estimates in Hereditary Nonpolyposis Colorectal Cancer: Are We There Yet?JNCI Cancer Spectr. 2020 Apr 27;4(5):pkaa030. doi: 10.1093/jncics/pkaa030. eCollection 2020 Oct. JNCI Cancer Spectr. 2020. PMID: 33134819 Free PMC article. No abstract available.
References
-
- Rustgi AK. The genetics of hereditary colon cancer. Genes Dev. 2007;21(20):2525-2538. - PubMed
-
- Provenzale D, Gupta S, Ahnen DJ, et al. Genetic/familial high-risk assessment: colorectal version 1.2016, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2016;14(8):1010-1030. - PubMed
-
- Vasen H, Watson P, Mecklin J, et al. New clinical criteria for hereditary nonpolyposis colorectal cancer (HNPCC, Lynch syndrome) proposed by the International Collaborative group on HNPCC. Gastroenterology. 1999;116(6):1453-1456. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous