

Stepwise segmentation error correction in optical coherence tomography angiography images of patients with diabetic macular edema
- PMID: 32923938
- PMCID: PMC7457684
- DOI: 10.1177/2515841420947931
Stepwise segmentation error correction in optical coherence tomography angiography images of patients with diabetic macular edema
Abstract
Aim: To determine the minimum number of optical coherence tomography B-scan corrections required to provide acceptable vessel density measurements on optical coherence tomography angiography images in eyes with diabetic macular edema.
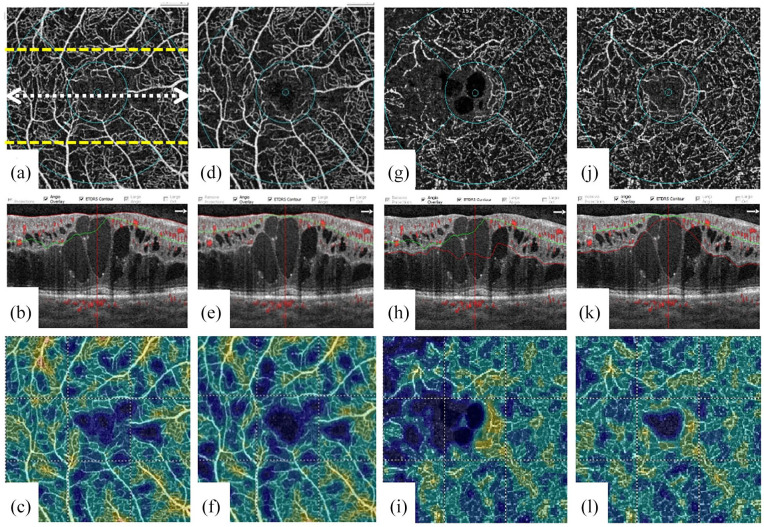
Methods: In this prospective, noninterventional case series, the optical coherence tomography angiography images of eyes with center-involving diabetic macular edema were assessed. Optical coherence tomography angiography imaging was performed using RTVue Avanti spectral-domain optical coherence tomography system with the AngioVue software (V.2017.1.0.151; Optovue, Fremont, CA, USA). Segmentation error was recorded and manually corrected in the inner retinal layers in the central foveal, 100th and 200th optical coherence tomography B-scans. The segmentation error correction was then continued until all optical coherence tomography B-scans in whole en face image were corrected. At each step, the manual correction of each optical coherence tomography B-scan was propagated to whole image. The vessel density and retinal thickness were recorded at baseline and after each optical coherence tomography B-scan correction.
Results: A total of 36 eyes of 26 patients were included. To achieve full segmentation error correction in whole en face image, an average of 1.72 ± 1.81 and 5.57 ± 3.87 B-scans was corrected in inner plexiform layer and outer plexiform layer, respectively. The change in the vessel density measurements after complete segmentation error correction was statistically significant after inner plexiform layer correction. However, no statistically significant change in vessel density was found after manual correction of the outer plexiform layer. The vessel density measurements were statistically significantly different after single central foveal B-scan correction of inner plexiform layer compared with the baseline measurements (p = 0.03); however, it remained unchanged after further segmentation corrections of inner plexiform layer.
Conclusion: Multiple optical coherence tomography B-scans should be manually corrected to address segmentation error in whole images of en face optical coherence tomography angiography in eyes with diabetic macular edema. Correction of central foveal B-scan provides the most significant change in vessel density measurements in eyes with diabetic macular edema.
Keywords: artifact; diabetic macular edema; optical coherence tomography angiography; segmentation error; vessel density.
© The Author(s), 2020.
Conflict of interest statement
Conflict of interest statement: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Segmentation Error Correction of the Optical Coherence Tomography Angiography Images in Peer-Reviewed Studies.J Curr Ophthalmol. 2022 Nov 30;34(3):273-276. doi: 10.4103/joco.joco_174_22. eCollection 2022 Jul-Sep. J Curr Ophthalmol. 2022. PMID: 36644458 Free PMC article. Review.
-
Effect of segmentation error correction on optical coherence tomography angiography measurements in healthy subjects and diabetic macular oedema.Br J Ophthalmol. 2020 Feb;104(2):162-166. doi: 10.1136/bjophthalmol-2019-314018. Epub 2019 Apr 29. Br J Ophthalmol. 2020. PMID: 31036586
-
MEASUREMENTS OF RETINAL FLUID BY OPTICAL COHERENCE TOMOGRAPHY LEAKAGE IN DIABETIC MACULAR EDEMA: A Biomarker of Visual Acuity Response to Treatment.Retina. 2019 Jan;39(1):52-60. doi: 10.1097/IAE.0000000000001905. Retina. 2019. PMID: 29077605
-
Macular vessels density in diabetic retinopathy: quantitative assessment using optical coherence tomography angiography.Int Ophthalmol. 2019 Aug;39(8):1845-1859. doi: 10.1007/s10792-018-1013-0. Epub 2018 Sep 7. Int Ophthalmol. 2019. PMID: 30194547
-
Inner Retinal Layer and Outer Retinal Layer Findings after Macular Hole Surgery Assessed by means of Optical Coherence Tomography.J Ophthalmol. 2019 Apr 1;2019:3821479. doi: 10.1155/2019/3821479. eCollection 2019. J Ophthalmol. 2019. PMID: 31061725 Free PMC article. Review.
Cited by
-
Segmentation Error Correction of the Optical Coherence Tomography Angiography Images in Peer-Reviewed Studies.J Curr Ophthalmol. 2022 Nov 30;34(3):273-276. doi: 10.4103/joco.joco_174_22. eCollection 2022 Jul-Sep. J Curr Ophthalmol. 2022. PMID: 36644458 Free PMC article. Review.
-
Sleeve gastrectomy improved microvascular phenotypes from obesity cohort, detected with optical coherence tomography angiography.J Diabetes. 2023 Apr;15(4):313-324. doi: 10.1111/1753-0407.13374. Epub 2023 Mar 5. J Diabetes. 2023. PMID: 36872300 Free PMC article.
-
Artifacts in Optical Coherence Tomography Angiography.J Ophthalmic Vis Res. 2021 Apr 29;16(2):271-286. doi: 10.18502/jovr.v16i2.9091. eCollection 2021 Apr-Jun. J Ophthalmic Vis Res. 2021. PMID: 34055264 Free PMC article. Review.
-
Application of Optical Coherence Tomography Angiography in True and Pseudo-Optic Disc Swelling.J Ophthalmol. 2024 Sep 30;2024:1164635. doi: 10.1155/2024/1164635. eCollection 2024. J Ophthalmol. 2024. PMID: 39380943 Free PMC article.
-
Microvascular Changes After Conbercept Intravitreal Injection of PDR With or Without Center-Involved Diabetic Macular Edema Analyzed by OCTA.Front Med (Lausanne). 2022 Mar 22;9:797087. doi: 10.3389/fmed.2022.797087. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35391880 Free PMC article.
References
-
- Han IC, Jaffe GJ. Evaluation of artifacts associated with macular spectral-domain optical coherence tomography. Ophthalmology 2010; 117: 1177–1189. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
