

Impact of right ventricular contractile reserve during low-load exercise on exercise intolerance in heart failure
- PMID: 32924319
- PMCID: PMC7755000
- DOI: 10.1002/ehf2.12968
Impact of right ventricular contractile reserve during low-load exercise on exercise intolerance in heart failure
Abstract
Aims: Traditional criteria for heart transplantation by cardiopulmonary exercise testing (CPX) include peak oxygen uptake (VO2 ) < 14 mL/kg/min. Reaching a sufficient exercise load is challenging for patients with refractory heart failure (HF) because of their exercise intolerance. Recently, a substantial impact of right ventricular (RV) dysfunction was highlighted on urgent heart transplantation and mortality. This study aims to investigate the impact of RV contractile reserve, assessed by low-load exercise stress echocardiography (ESE), on exercise intolerance defined as peak VO2 < 14 mL/kg/min, in patients with HF.
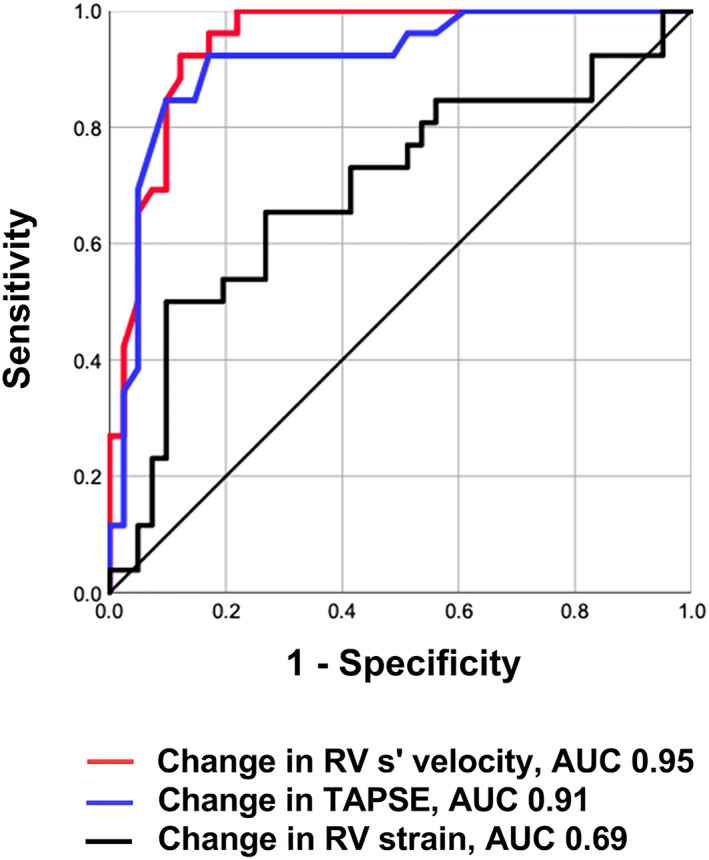
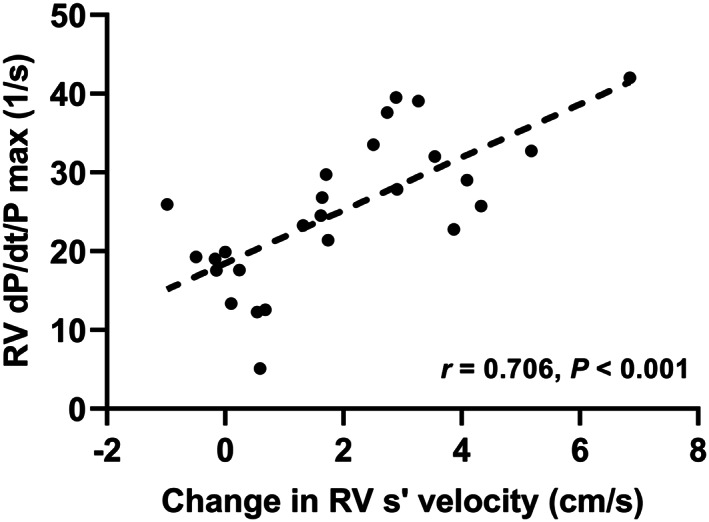
Methods and results: We prospectively examined 67 consecutive patients hospitalized for HF who underwent ESE and CPX under a stabilized HF condition. Although low-load ESE was defined as 25 W load exercise, an increment in RV systolic (s') velocity was regarded as the preservation of RV contractile reserve. All patients completed low-load ESE. During low-load ESE, the variation in RV s' velocity significantly correlated with peak VO2 (r = 0.787, P < 0.001). The change in RV s' velocity during low-load ESE accurately identified patients with peak VO2 < 14 mL/kg/min (area under the curve, 0.95; sensitivity, 92%; specificity, 85%). The intraclass correlation coefficient for intra-observer and inter-observer agreement for the change in RV s' velocity was 0.96 (95% confidence interval, 0.88-0.99, P < 0.001) and 0.86 (95% confidence interval, 0.64-0.95, P < 0.001), respectively. The RV-to-pulmonary circulation (PC) coupling, which was assessed by the slope of the relationship between RV s' velocity and pulmonary artery systolic pressure at rest and low-load exercise, was worse in the low-peak VO2 group (<14 mL/kg/min) than the preserved-peak VO2 group (≥14 mL/kg/min).
Conclusions: The change in RV s' velocity during low-load ESE could estimate the exercise capacity in HF patients. The assessments of RV contractile reserve and RV-to-PC coupling could be clinically beneficial to distinguish high-risk HF patients.
Keywords: cardiopulmonary exercise testing; exercise stress echocardiography; heart failure; low-load exercise; right ventricular contractile reserve; right ventricular-to-pulmonary circulation coupling.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
None declared.
Figures



References
-
- Weber KT, Kinasewitz GT, Janicki JS, Fishman AP. Oxygen utilization and ventilation during exercise in patients with chronic cardiac failure. Circulation 1982; 65: 1213–1223. - PubMed
-
- Adachi H. Cardiopulmonary exercise test. Int Heart J 2017; 58: 654–665. - PubMed
-
- Mancini DM, Eisen H, Kussmaul W, Mull R, Edmonds LH, Wilson JR. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation 1991; 83: 778–786. - PubMed
-
- Mudge GH, Goldstein S, Addonizio LJ, Caplan A, Mancini D, Levine TB, Ritsch ME, Stevenson LW. Task force 3: recipient guidelines/prioritization. J Am Coll Cardiol 1993; 22: 21–31. - PubMed
-
- Frea S, Pidello S, Bovolo V, Iacovino C, Franco E, Pinneri F, Galluzzo A, Volpe A, Visconti M, Peirone A, Morello M, Bergerone S, Gaita F. Prognostic incremental role of right ventricular function in acute decompensation of advanced chronic heart failure. Eur J Heart Fail 2016; 18: 564–572. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous