

Reduced Monocytic Human Leukocyte Antigen-DR Expression Indicates Immunosuppression in Critically Ill COVID-19 Patients
- PMID: 32925314
- PMCID: PMC7288784
- DOI: 10.1213/ANE.0000000000005044
Reduced Monocytic Human Leukocyte Antigen-DR Expression Indicates Immunosuppression in Critically Ill COVID-19 Patients
Abstract
Background: The cellular immune system is of pivotal importance with regard to the response to severe infections. Monocytes/macrophages are considered key immune cells in infections and downregulation of the surface expression of monocytic human leukocyte antigen-DR (mHLA-DR) within the major histocompatibility complex class II reflects a state of immunosuppression, also referred to as injury-associated immunosuppression. As the role of immunosuppression in coronavirus disease 2019 (COVID-19) is currently unclear, we seek to explore the level of mHLA-DR expression in COVID-19 patients.
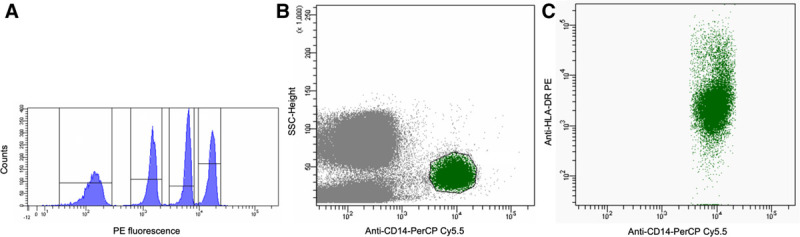
Methods: In a preliminary prospective monocentric observational study, 16 COVID-19-positive patients (75% male, median age: 68 [interquartile range 59-75]) requiring hospitalization were included. The median Acute Physiology and Chronic Health Evaluation-II (APACHE-II) score in 9 intensive care unit (ICU) patients with acute respiratory failure was 30 (interquartile range 25-32). Standardized quantitative assessment of HLA-DR on monocytes (cluster of differentiation 14+ cells) was performed using calibrated flow cytometry at baseline (ICU/hospital admission) and at days 3 and 5 after ICU admission. Baseline data were compared to hospitalized noncritically ill COVID-19 patients.
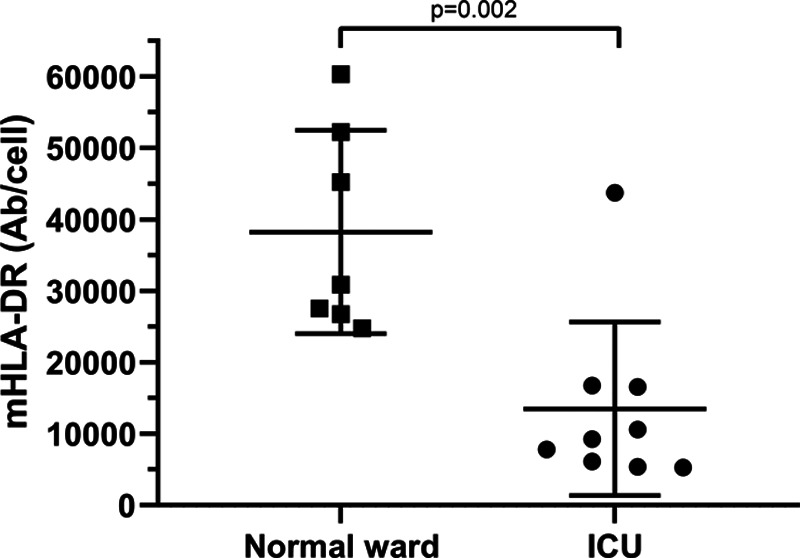
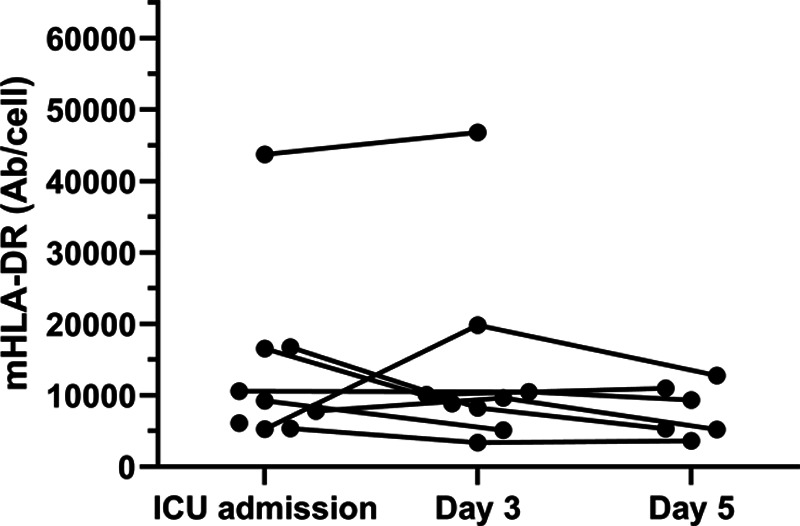
Results: While normal mHLA-DR expression was observed in all hospitalized noncritically ill patients (n = 7), 89% (8 of 9) critically ill patients with COVID-19-induced acute respiratory failure showed signs of downregulation of mHLA-DR at ICU admission. mHLA-DR expression at admission was significantly lower in critically ill patients (median, [quartiles]: 9280 antibodies/cell [6114, 16,567]) as compared to the noncritically ill patients (30,900 antibodies/cell [26,777, 52,251]), with a median difference of 21,508 antibodies/cell (95% confidence interval [CI], 14,118-42,971), P = .002. Reduced mHLA-DR expression was observed to persist until day 5 after ICU admission.
Conclusions: When compared to noncritically ill hospitalized COVID-19 patients, ICU patients with severe COVID-19 disease showed reduced mHLA-DR expression on circulating CD14+ monocytes at ICU admission, indicating a dysfunctional immune response. This immunosuppressive (monocytic) phenotype remained unchanged over the ensuing days after ICU admission. Strategies aiming for immunomodulation in this population of critically ill patients should be guided by an immune-monitoring program in an effort to determine who might benefit best from a given immunological intervention.
Conflict of interest statement
Conflicts of Interest: See Disclosures at the end of the article.
Figures
Comment in
-
Human Leukocyte Antigen-DR Deficiency and Immunosuppression-Related End-Organ Failure in SARS-CoV2 Infection.Anesth Analg. 2020 Oct;131(4):989-992. doi: 10.1213/ANE.0000000000005140. Anesth Analg. 2020. PMID: 32925313 Free PMC article. No abstract available.
References
-
- Rieckmann JC, Geiger R, Hornburg D. Social network architecture of human immune cells unveiled by quantitative proteomics. Nat Immunol. 2017;18:583–593. - PubMed
-
- Rubio I, Osuchowski MF, Shankar-Hari M. Current gaps in sepsis immunology: new opportunities for translational research. Lancet Infect Dis. 2019;19:e422–e436. - PubMed
-
- Schefold JC, Hasper D, Reinke P, Monneret G, Volk HD. Consider delayed immunosuppression into the concept of sepsis. Crit Care Med. 2008;36:3118. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
