

Prediction of Opioid-Induced Respiratory Depression on Inpatient Wards Using Continuous Capnography and Oximetry: An International Prospective, Observational Trial
- PMID: 32925318
- PMCID: PMC7467153
- DOI: 10.1213/ANE.0000000000004788
Prediction of Opioid-Induced Respiratory Depression on Inpatient Wards Using Continuous Capnography and Oximetry: An International Prospective, Observational Trial
Abstract
Background: Opioid-related adverse events are a serious problem in hospitalized patients. Little is known about patients who are likely to experience opioid-induced respiratory depression events on the general care floor and may benefit from improved monitoring and early intervention. The trial objective was to derive and validate a risk prediction tool for respiratory depression in patients receiving opioids, as detected by continuous pulse oximetry and capnography monitoring.
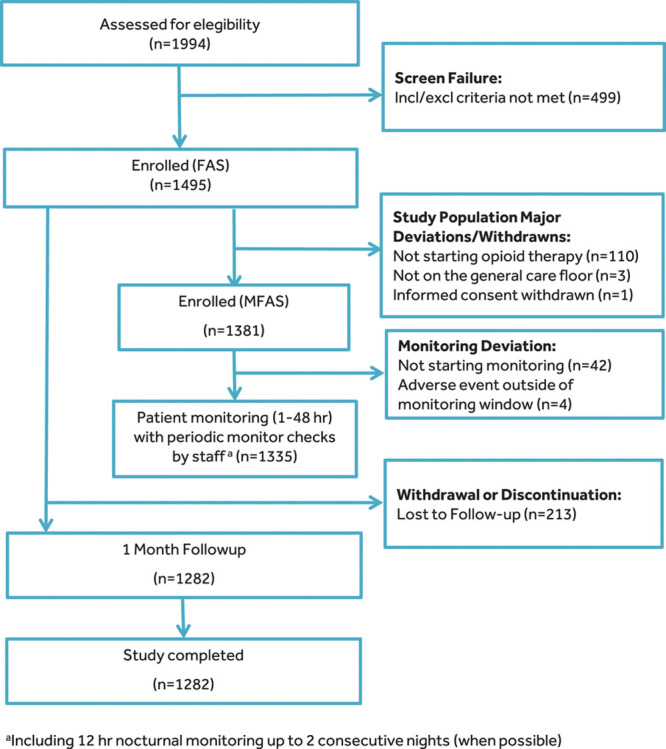
Methods: PRediction of Opioid-induced respiratory Depression In patients monitored by capnoGraphY (PRODIGY) was a prospective, observational trial of blinded continuous capnography and oximetry conducted at 16 sites in the United States, Europe, and Asia. Vital signs were intermittently monitored per standard of care. A total of 1335 patients receiving parenteral opioids and continuously monitored on the general care floor were included in the analysis. A respiratory depression episode was defined as respiratory rate ≤5 breaths/min (bpm), oxygen saturation ≤85%, or end-tidal carbon dioxide ≤15 or ≥60 mm Hg for ≥3 minutes; apnea episode lasting >30 seconds; or any respiratory opioid-related adverse event. A risk prediction tool was derived using a multivariable logistic regression model of 46 a priori defined risk factors with stepwise selection and was internally validated by bootstrapping.
Results: One or more respiratory depression episodes were detected in 614 (46%) of 1335 general care floor patients (43% male; mean age, 58 ± 14 years) continuously monitored for a median of 24 hours (interquartile range [IQR], 17-26). A multivariable respiratory depression prediction model with area under the curve of 0.740 was developed using 5 independent variables: age ≥60 (in decades), sex, opioid naivety, sleep disorders, and chronic heart failure. The PRODIGY risk prediction tool showed significant separation between patients with and without respiratory depression (P < .001) and an odds ratio of 6.07 (95% confidence interval [CI], 4.44-8.30; P < .001) between the high- and low-risk groups. Compared to patients without respiratory depression episodes, mean hospital length of stay was 3 days longer in patients with ≥1 respiratory depression episode (10.5 ± 10.8 vs 7.7 ± 7.8 days; P < .0001) identified using continuous oximetry and capnography monitoring.
Conclusions: A PRODIGY risk prediction model, derived from continuous oximetry and capnography, accurately predicts respiratory depression episodes in patients receiving opioids on the general care floor. Implementation of the PRODIGY score to determine the need for continuous monitoring may be a first step to reduce the incidence and consequences of respiratory compromise in patients receiving opioids on the general care floor.
Trial registration: ClinicalTrials.gov NCT02811302.
Conflict of interest statement
Funding: This work was supported by Medtronic. All authors have completed the International Committee of Medical Journal Editors (ICMJE) Form for Disclosure of Potential Conflicts of Interest. All authors except P.D.S. report financial support to the Investigator or Investigator’s Institution to fund the Medtronic-sponsored trial, as well as medical writing and editorial support by a medical writer employed by Medtronic.
Conflicts of Interest: See Disclosures at the end of the article.
Figures
Comment in
-
Postoperative Opioid-Induced Respiratory Depression: 3 Steps Forward.Anesth Analg. 2020 Oct;131(4):1007-1011. doi: 10.1213/ANE.0000000000005098. Anesth Analg. 2020. PMID: 32925317 No abstract available.
-
PRODIGY Score and Post-hoc Analysis of Previous Studies of Postoperative Respiratory Depression.Anesth Analg. 2021 Mar 1;132(3):e44-e45. doi: 10.1213/ANE.0000000000005339. Anesth Analg. 2021. PMID: 33591102 No abstract available.
-
In Response.Anesth Analg. 2021 Mar 1;132(3):e45-e46. doi: 10.1213/ANE.0000000000005340. Anesth Analg. 2021. PMID: 33591103 No abstract available.
-
Opioid-Induced Respiratory Depression: Is Hydromorphone Safer Than Morphine?Anesth Analg. 2021 Apr 1;132(4):e60. doi: 10.1213/ANE.0000000000005413. Anesth Analg. 2021. PMID: 33723198 No abstract available.
-
In Response.Anesth Analg. 2021 Apr 1;132(4):e61. doi: 10.1213/ANE.0000000000005415. Anesth Analg. 2021. PMID: 33723199 No abstract available.
References
-
- Khanna AK, Overdyk FJ, Greening C, Di Stefano P, Buhre WF. Respiratory depression in low acuity hospital settings-seeking answers from the PRODIGY trial. J Crit Care. 2018;47:80–87. - PubMed
-
- Andersen LW, Berg KM, Chase M, Cocchi MN, Massaro J, Donnino MW; American Heart Association’s Get With The Guidelines(®)-Resuscitation Investigators. Acute respiratory compromise on inpatient wards in the United States: incidence, outcomes, and factors associated with in-hospital mortality. Resuscitation. 2016;105:123–129. - PubMed
-
- Jarzyna D, Jungquist CR, Pasero C, et al. American Society for Pain Management Nursing guidelines on monitoring for opioid-induced sedation and respiratory depression. Pain Manag Nurs. 2011;12:118–145.e10. - PubMed
-
- DeVita MA, Smith GB, Adam SK, et al. “Identifying the hospitalised patient in crisis”–a consensus conference on the afferent limb of rapid response systems. Resuscitation. 2010;81:375–382. - PubMed
