

Impact of a pay-for-performance scheme for long-acting reversible contraceptive (LARC) advice on contraceptive uptake and abortion in British primary care: An interrupted time series study
- PMID: 32925909
- PMCID: PMC7489538
- DOI: 10.1371/journal.pmed.1003333
Impact of a pay-for-performance scheme for long-acting reversible contraceptive (LARC) advice on contraceptive uptake and abortion in British primary care: An interrupted time series study
Abstract
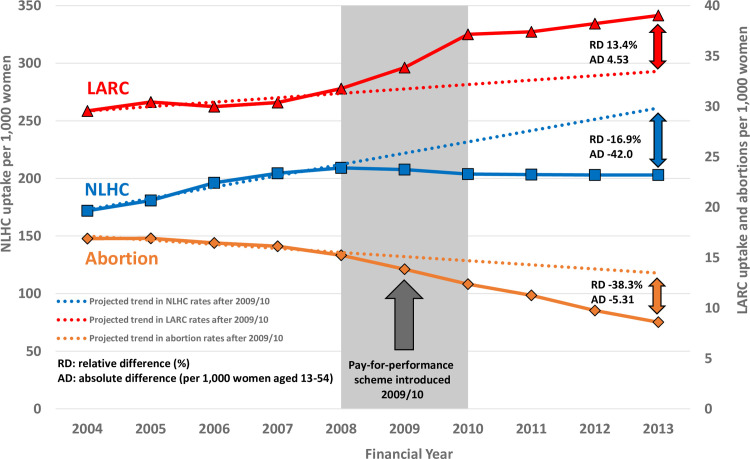
Background: Long-acting reversible contraception (LARC) is among the most effective contraceptive methods, but uptake remains low even in high-income settings. In 2009/2010, a target-based pay-for-performance (P4P) scheme in Britain was introduced for primary care physicians (PCPs) to offer advice about LARC methods to a specified proportion of women attending for contraceptive care to improve contraceptive choice. We examined the impact and equity of this scheme on LARC uptake and abortions.
Methods and findings: We examined records of 3,281,667 women aged 13 to 54 years registered with a primary care clinic in Britain (England, Wales, and Scotland) using Clinical Practice Research Datalink (CPRD) from 2004/2005 to 2013/2014. We used interrupted time series (ITS) analysis to examine trends in annual LARC and non-LARC hormonal contraception (NLHC) uptake and abortion rates, stratified by age and deprivation groups, before and after the P4P was introduced in 2009/2010. Between 2004/2005 and 2013/2014, crude LARC uptake rates increased by 32.0% from 29.6 per 1,000 women to 39.0 per 1,000 women, compared with 18.0% decrease in NLHC uptake. LARC uptake among women of all ages increased immediately after the P4P with step change of 5.36 per 1,000 women (all values are per 1,000 women unless stated, 95% CI 5.26-5.45, p < 0.001). Women aged 20 to 24 years had the largest step change (8.40, 8.34-8.47, p < 0.001) and sustained trend increase (3.14, 3.08-3.19, p < 0.001) compared with other age groups. NLHC uptake fell in all women with a step change of -22.8 (-24.5 to -21.2, p < 0.001), largely due to fall in combined hormonal contraception (CHC; -15.0, -15.5 to -14.5, p < 0.001). Abortion rates in all women fell immediately after the P4P with a step change of -2.28 (-2.98 to -1.57, p = 0.002) and sustained decrease in trend of -0.88 (-1.12 to -0.63, p < 0.001). The largest falls occurred in women aged 13 to 19 years (step change -5.04, -7.56 to -2.51, p = 0.011), women aged 20 to 24 years (step change -4.52, -7.48 to -1.57, p = 0.030), and women from the most deprived group (step change -4.40, -6.89 to -1.91, p = 0.018). We estimate that by 2013/2014, the P4P scheme resulted in an additional 4.53 LARC prescriptions per 1,000 women (relative increase of 13.4%) more than would have been expected without the scheme. There was a concurrent absolute reduction of -5.31 abortions per 1,000 women, or -38.3% relative reduction. Despite universal coverage of healthcare, some women might have obtained contraception elsewhere or had abortion procedure that was not recorded on CPRD. Other policies aiming to increase LARC use or reduce unplanned pregnancies around the same time could also explain the findings.
Conclusions: In this study, we found that LARC uptake increased and abortions fell in the period after the P4P scheme in British primary care, with additional impact for young women aged 20-24 years and those from deprived backgrounds.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: RM is an NHS general practitioner, and his practice receives funding for achieving P4P targets. His practice receives extra funding for providing a LARC service for patients registered with his practice. He has also received honoraria for writing commissioned articles for magazines and lectures at educational events paid directly by publishers or organisers of meetings but not directly by pharma. EC has nothing to disclose. AB reports grants from Dr Foster outside the submitted work. RF reports personal fees from Natural Cycles outside the submitted work. SS reports grants from NIHR School for Public Health Research, grants from NIHR Collaboration for Applied Research Collaboration North West London, during the conduct of the study; and grants from The Daily Mile Foundation, outside the submitted work; SS is an NHS general practitioner, and her practice receives funding for achieving P4P targets.
Figures
References
-
- National Statistics. Abortion Statistics England and Wales 2018. Department of Health and Social Care, 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
